This paper discusses the role of positive deviance (PD) in achieving safety. They start by talking about many existing safety approaches (in healthcare) feel like a “relentlessly negative treadmill” (p880) with incident investigations, audits and other activities focusing most attention on what goes wrong and how often, why errors occur, and “who or what is at the root of the problem” (p880).
They say that these find-and-fix approaches mostly tell us about the absence of safety instead of its presence. Instead, “These efforts aim to prevent harm by striving to reduce the number of things that go wrong,1 as opposed to identifying instances when—often despite challenging circumstances and limited resources—things go right” (p880) and according to the research they’ve cited, hasn’t produced the expected gains in patient safety. It’s argued the main focus on error ID hasn’t resulted in expected gains in patient safety because it’s not well-suited to complex systems.
Instead, they say that behaviours producing variability are the same processes that produce success, so focusing on successful practices may be an effective tactic to add. One approach to focus on success is positive deviance (PD).
PD posits that workplaces tend to have individuals/teams that maintain successful work or exceptional performance and solve common problems using (sometimes) uncommon methods. That is, PD are the individuals or groups that have pockets of excellence or high performance and especially under trying conditions.
The paper argues that medicine (but likely most industries) focus more on identifying/eliminating negative events or problems to fix, rather than identifying and spreading successful practices. Because solutions to problems are generated within the same community, they may be more readily adopted elsewhere.
Despite some of these PD initiatives in healthcare apparently having “the potential to save lives” (p881), the main focus has been on negative deviance (eg finding problems & root causes) rather than identifying effective practices. They provide several reasons why this may be.
One reason may be that “the consistent delivery of well-executed safe care under typically difficult circumstances tends to go unrecognised” (p881); that is, safe, effective & reliable work tends to be invisible.
Another reason may be the human need to look for problems to fix rather than the more unusual “recognise and spread success“ (p881). Another may be the difficulty in attracting role models, or in other cases the organisational power differentials may inhibit open learning (e.g. between doctors and nurses). In some cases, there may be temptations to “shield knowledge in pursuit of selfinterest due to, for example, provider organisations who feel they are in competition for local resources, or staff who feel insecure about their job due to efficiency drives (p881).
Authors suggest four steps in the PD approach:
1. Identify PDs
2. Study PDs in-depth
3. Micro-experiments of practices
4. Disseminate practices via collaboration
They briefly cover research highlighting how PD approaches have been used and how effective they were. In one instance using a PD approach (eg identifying the PDs, understanding how top performance is achieved, statistically testing the hypothesis for top performance, working with key stakeholders and adopters to disseminate the practice), it was found that performance increased from 50% to 75% in hospital meetings meeting the 90-min guidelines. Other examples around hand washing and more were cited.
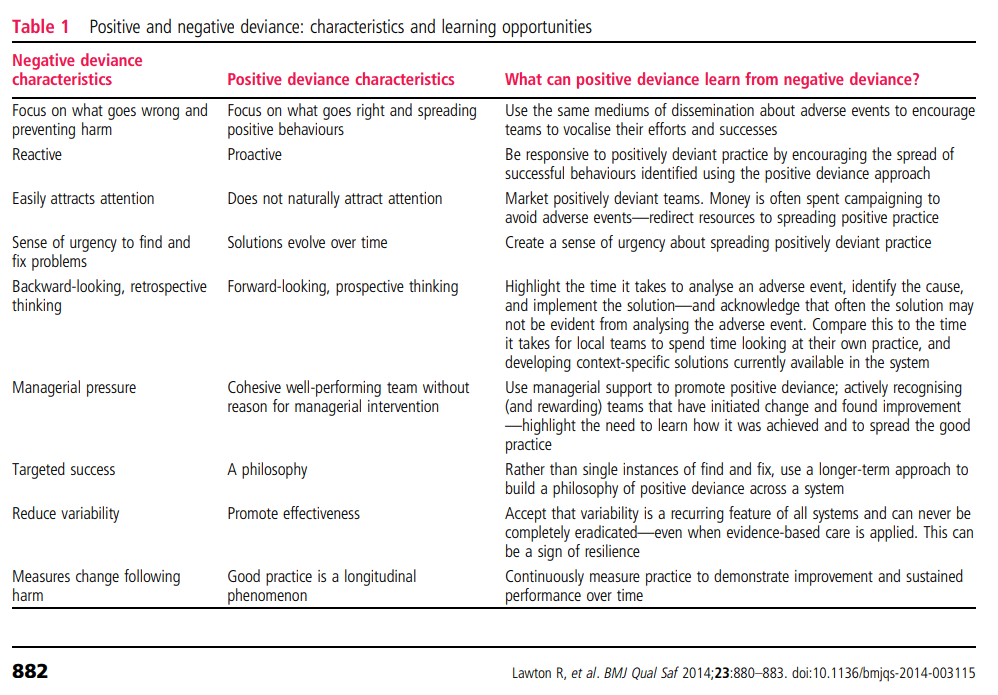
Increasing the difficulty of PD approaches is that following the aftermath of adverse events, there is typically a real drive to mobilise attention, managerial resources and a sense of urgency. This combination to find and fix problems may be lacking in the case of positive deviance because a “cohesive and well-performing team is unlikely to create managerial attention, as the positive practices may have simply evolved over time” (p882).
The authors suggest that drawing on the negative deviance strategies to improve PD may include: (p882)
- allocating resources usually focussed on reporting and reducing error to spreading positive behaviours,
- recognising positively deviant teams, and
- creating a sense of urgency about spreading positive exemplars of practice.
The authors conclude that since most focus is placed on responding to adverse events (which is still critical), it belies the fact that most of the time and operating under time-pressured and resource-constrained complex uncertain environments, things tend to go very right most of the time.
Thus, quoting the authors, now “is the time to send more optimistic signals to clinicians, focusing on the behaviours, processes and systems contributing to resilient, safe care” (p882). It’s advised that a sense of urgency should be created to spread positively deviant practice, given its proactive focus.
Examples below of how the shift from negative deviance to PD can be achieved.
Authors: Rebecca Lawton, Natalie Taylor, Robyn Clay-Williams, Jeffrey Braithwaite, 2014, BMJ Quality & Safety
Study link: http://dx.doi.org/10.1136/bmjqs-2014-003115
Link to the LinkedIn article: https://www.linkedin.com/pulse/positive-deviance-different-approach-achieving-safety-ben-hutchinson
