This study evaluated 41 maritime accident reports relating to machinery space fires and explosions. The goal was to determine if organisational factors are identified during the accident investigations.
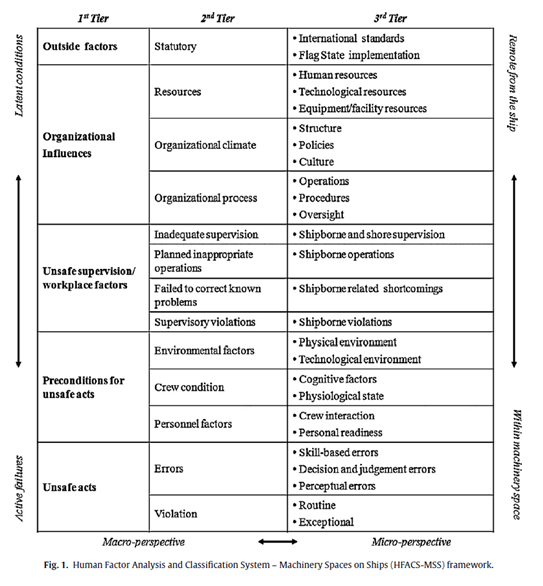
A modified HFACS was used to evaluate the accident reports (Human Factor Analysis and Classification System, shown below).
[Note: Like with any accident evaluation method – what-you-look-for-is-what-you-find. This is just as applicable to HFACS as it is to more systems-focused methods (STAMP/CAST, AcciMap, EAST etc.). This is recognised by the authors, and thus, they didn’t try to validate the causal/contributory factors but rather categorise what was described in the reports.]
I’ve skipped the majority of the findings relating to contributory factor breakdown percentages.
Results
A key, but perhaps not surprising finding, is that “organizational factors were not identified by maritime accident investigators to the extent expected had the IMO guidelines been observed. Instead, contributing factors at the lower end of organizational echelons are over-represented” (p1187).
For instance:
- 3.5% reports identified statutory factors
- 13.9% organisational factors
- 1.1% organisational climate and 5.7% organisational processes
- 5.7% unsafe supervision
- 56.5% preconditions for unsafe acts
- 20.4% unsafe acts
More latent conditions higher on the HFACS levels were represented substantially less than more active failures (e.g. preconditions for unsafe acts rated highly). Indeed, “All 41 accident investigation reports contained preconditions for unsafe acts as contributing factors” (p1191).
While interaction with technology ranked highly (41.3% of reports), this was under the level of “preconditions for unsafe acts”, so at the sharper end rather than upstream design and organisational levels.
18 reports identified organisational influences. 12 of these 18 reports further identified organisational climate, but did not explain or “reveal why this conclusion was made in the accident investigation and what effects the organizational contribution had on lower HFACS levels in the course of the development of the accident” (p1192).
Another interesting observation is that while a large number of preconditions for unsafe acts were highlighted, “many of the identified organizational influences [identified in the investigation reports] did not seem to relate to the accident investigation reviewed” (p1194).
While technology at the lower levels was identified frequently, what isn’t readily identified is how far the organisational arrangements influenced those technical failures. Notably, “the accident investigation reports seem to neglect the societal component of safety-critical systems. This is not meant to say that technological components are not important aspects of socio-organizational systems” (p1194).
Some examples are provided below, where the authors select some findings from accident reports (left column) and then dive deeper into possible upstream/organisational influences (right column) that were not covered or explored in the reports.
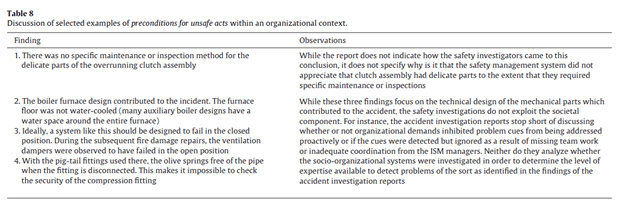
While the authors do not try to second-guess the investigation reports or counter the logics of the findings, it’s highlighted that without an evaluation of broader reasons *how* the apparent “preconditions for unsafe acts” or technology issues existed without evaluating upstream or broader factors seems to imply that organisations are missing out on key intel.
In saying this, the difficulty in exploring socio-technical factors is recognised as anything but “a clear-cut task” (p1194). Another study identified six levels of actors who influenced “normal work process[es] and (therefore accident scenarios)” and these levels ranked from micro work & technological levels through to macro (government/statutory) levels.
The near absence of higher-level factors in these accident reports was argued to be limiting in understanding the events in their context. Drawing on other research, it’s argued investigations should, at the least consider:
- The pre-accident historical background; capturing the circumstances around which the system deteriorated over time
- The specific conditions in the organisational context which influenced and provided the conditions for the deterioration
Finally, it’s nicely argued that while the accident investigation reports were likely not trying to directly apportion blame on downstream actors, “the (excessive) focus of these accident investigation reports on unsafe acts ‘committed’ by the sharp end is not reflecting this at all” (p1196). Further, “Even if these reports do not incite legal concepts of recklessness, carelessness and fault”, the relentless focus on frontline issues by proxy “is implying fault, albeit not from a legal perspective” (p1196).
These unintended attributions of fault, “[are] subjective at best and a social judgment rather than a scientific conclusion based on the holistic analysis of the socio-organization under investigation” (p1196).
Authors: Jens U. Schröder-Hinrichs∗, Michael Baldauf, Kevin T. Ghirxi, 2011, Safety Science
Study link: https://doi.org/10.1016/j.aap.2010.12.033
Link to the LinkedIn article: https://www.linkedin.com/pulse/accident-investigation-reporting-deficiencies-related-ben-hutchinson

One thought on “Accident investigation reporting deficiencies related to organizational factors in machinery space fires and explosions”