ABSTRACT
Study Objectives
The amount of recovery sleep needed to fully restore well-established neurobehavioral deficits from sleep loss remains unknown, as does whether the recovery pattern differs across measures after total sleep deprivation (TSD) and chronic sleep restriction (SR).
Methods
In total, 83 adults received two baseline nights (10–12-hour time in bed [TIB]) followed by five 4-hour TIB SR nights or 36-hour TSD and four recovery nights (R1–R4; 12-hour TIB). Neurobehavioral tests were completed every 2 hours during wakefulness and a Maintenance of Wakefulness Test measured physiological sleepiness. Polysomnography was collected on B2, R1, and R4 nights.
Results
TSD and SR produced significant deficits in cognitive performance, increases in self-reported sleepiness and fatigue, decreases in vigor, and increases in physiological sleepiness. Neurobehavioral recovery from SR occurred after R1 and was maintained for all measures except Psychomotor Vigilance Test (PVT) lapses and response speed, which failed to completely recover. Neurobehavioral recovery from TSD occurred after R1 and was maintained for all cognitive and self-reported measures, except for vigor. After TSD and SR, R1 recovery sleep was longer and of higher efficiency and better quality than R4 recovery sleep.
Conclusions
PVT impairments from SR failed to reverse completely; by contrast, vigor did not recover after TSD; all other deficits were reversed after sleep loss. These results suggest that TSD and SR induce sustained, differential biological, physiological, and/or neural changes, which remarkably are not reversed with chronic, long-duration recovery sleep. Our findings have critical implications for the population at large and for military and health professionals.
*****************************************************************************
From the full-text paper:
Another interesting study which explored the impact of both total sleep deprivation (TSD; staying awake during normal sleep periods) and chronic sleep restriction (SR; smaller amounts of sleep lost per sleep period over a longer period) on the recovery time in psychomotor vigilance (reaction time tests), a maintenance of wakefulness test (to measure physiological sleepiness), subjective sleepiness and polysomnography.
Namely, they restricted the time in bed to either 4 hours per night over 5 nights or a complete sleep restriction period of 36 hours, followed by 4 nights of recovery sleep (12 hour time in bed).
Results:
- As expected, TSD and SR both produced significant reductions in cognitive performance, increased self-reported sleepiness and fatigue, reduced vigour and increased physiological sleepiness.
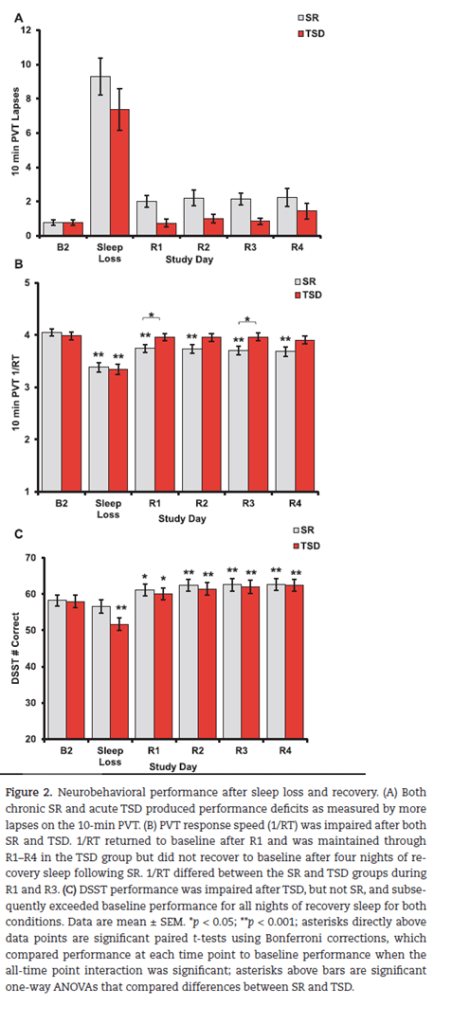
- Most interesting is that even after four nights of recovery sleep the psychomotor vigilance performance (both lapses and reaction speed) had not fully recovered.
- They conclude that “both SR and TSD produce chronic and sustained biological, physiological, and/or neural changes reflected in neurobehavioral measures” and that even “12-hour [time in bed] recovery across four consecutive nights is, notably, not enough to reverse these alterations” (p8).
- Following SR, self-reported deficits and physiological sleepiness were reversed after the recovery period. Moreover after TSD cognitive performance, physiological and self-rated sleepiness and self-reported fatigue recovery occurred rapidly, but perceptions of decreased subjective vigour “lingered after four recovery nights”.
- On the above, vigour returned to baseline over 3 of the 4 recovery nights but then significantly decreased again on the 4th night of recovery. They suggest that this relayed effect may be due to lingering instability of vigour caused by prior sleep loss or maybe “individuals may have initially reported increased vigor due to comparing their perceptions to those during sleep loss. However, as recovery progressed, individuals may have altered their perception comparison anchor to baseline and thus reported decreased vigor” (p8).
- They note several limitations of the study. One is the participants were healthy young adults without reported sleep, mood or medical conditions. Adolescents, middle-aged and older individuals may show different recovery responses. Also, no control group was employed so any natural variations in sleep stability could not be compared.
- The image below was modified from the paper and shows some of the cognitive performance data.
These results largely support other research finding that chronic sleep restriction may take far more time for full recovery than usually permitted in our lifestyles and work-life conditions.
Authors: Erika M Yamazaki, Caroline A Antler, Charlotte R Lasek, Namni Goel. Sleep, Volume 44, Issue 4, April 2021.
Study link: https://doi.org/10.1093/sleep/zsaa224
Another study looking at sleep loss and recovery: https://www.linkedin.com/posts/benhutchinson2_how-hazardous-is-sleep-loss-for-safety-comparable-activity-6917253256897318912-DNJj?utm_source=linkedin_share&utm_medium=member_desktop_web
Link to the LinkedIn article: https://www.linkedin.com/feed/update/urn:li:ugcPost:6929196435070476288?updateEntityUrn=urn%3Ali%3Afs_updateV2%3A%28urn%3Ali%3AugcPost%3A6929196435070476288%2CFEED_DETAIL%2CEMPTY%2CDEFAULT%2Cfalse%29

One thought on “Residual, differential neurobehavioral deficits linger after multiple recovery nights following chronic sleep restriction or acute total sleep deprivation”