This explored the extent and nature of blame in family practice safety incident reports. 2148 incident reports from a database of 14 million reports was analysed.
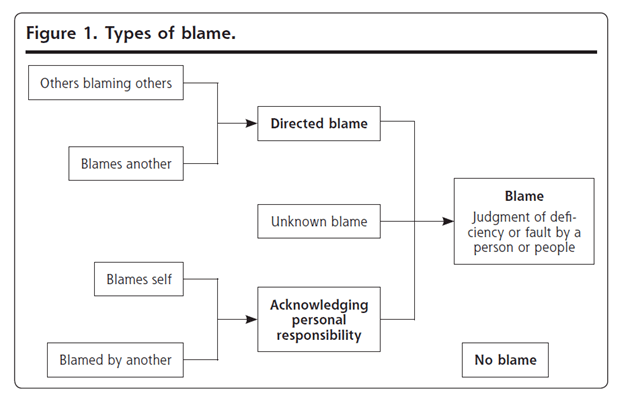
Blame was defined as “evidence in the free-text of a judgement about a deficiency or fault by a person or people” (p457).
Problems exist with current approaches to incident identification and learning. For instance, previous research suggested that perhaps only 1 in 10 adverse events in hospitals are formally reported; where “underreporting is the norm” (p455).
The patient safety movement is predicated that these types of harm events are largely the result of poorly designed systems. Even so, other research highlights that incident reports frequently highlight faults of people and decisions rather than “considering system failings” (p455).
Primary care is said to lag secondary care in generating learning from incidents and also has other challenges that may not be quite as prominent in hospitals, for instance, whistleblowing and reporting practices of others may be exceedingly difficult in a family practice within a small clinical team.
Fear of being held personally accountable is believed to be a major factor in reluctance for staff to report incidents; blame is known to hinder reporting.
Results
Key findings were that: blame was present in 45% of reports. In 36% of cases, those who reported the incidents attributed the fault to other people whereas in only 2% of cases did the person reporting the event acknowledge personal responsibility.
They state that because “42% of reports were used to censure others” this suggests that “progress toward a blame-free and supportive culture is slow” (p459). Moreover, directed blame reports were more likely in response to or anticipation of a complaint (e.g. by patients, family, other staff etc.)
Five categories of blame were found in the sample of reports: 1. acknowledging personal responsibility (blaming self), 2. directed blame at another person, 3. others blaming others, 4. unknown blame, 5. no blame.
The 3 types of incidents most likely associated with directed blame were discharge planning, communication problems and referrals.
In contrast, reports involving record keeping and documentation and pressure ulcers were less likely to have directed blame at others. Directed blame was less likely in cases where patients were harmed (except for deaths).
The former factors involve more clinical judgement and interactions with patients and other stakeholders, so therefore more uncertainty and variability (and thus blame) is associated, whereas the latter factors like pressure ulcers are more “matter of fact” and less prone to misinterpretation.
What I found most interesting is:
- when reports described 1 or more contributing factors, they were more likely to associate directed blame (50% of reports) compared to when contributing factors weren’t identified (36% of cases).
- Reports listing organisational factors had higher odds of apportioning directed blame at people, leading the authors to posit that perhaps “those reporting incidents may still make fundamental attribution errors despite recognizing system factors assessment” (p459).
These results hint that these care environments prioritise allocating personal accountability over effective and systematic learning.
Fundamental attribution error may be a strong factor in explaining these findings. People are more likely to appreciate systems factors in understanding their own actions but focus more on personal/individual factors when explaining actions of others. This may partially explain why those reporting incidents recognised personal accountability in just 2% of cases, compared with 42% directing blame at others.
On the point of fundamental attribution error, it’s possible that the voices of those most directly connected to the events aren’t having an active enough presence in the post-event learning process. Thus, “We may be missing key insights and soft intelligence that individuals closest to these incidents might have offered” (p459).
[** I see this a lot in other industries like construction, where the person most directly involved in an event is almost treated like a criminal witness and their words and accounts of the event are scrutinised against other stakeholders.]
It’s said that soft intelligence, that is the insights of experiences from frontline staff about the reality of the system, “can thrive only where staff feel valued and respected” (p459).
Unfortunately, incident reporting & investigation have a long and depressing history of not providing “this soft intelligence or support[ing] this ethic” (p459).
Concluding, they argue that the “high frequency of blame in these safety, incident reports may reflect a health care culture that leads to blame and retribution, rather than to identifying areas for learning and improvement, and a failure to appreciate the contribution of system factors in others’ behavior” (p455).
Authors: Cooper, J., Edwards, A., Williams, H., Sheikh, A., Parry, G., Hibbert, P., … & Carson-Stevens, A. (2017). The Annals of Family Medicine, 15(5), 455-461.

Study link: https://doi.org/10.1370/afm.2123
Link to the LinkedIn article: https://www.linkedin.com/pulse/nature-blame-patient-safety-incident-reports-mixed-ben-hutchinson

2 thoughts on “Nature of Blame in Patient Safety Incident Reports: Mixed methods analysis of a national database”