This explored the impact that critical events have on healthcare staff and how they “move on” from the events via interviews, memos and field notes. The ‘second victim’ lens was used to situate the findings.
Critical events are “’a sudden unexpected event that has an emotional impact sufficient to overwhelm the usually effective coping skills of an individual and cause significant psychological stress” (p2). These events can lead to extreme emotional suffering for staff and impact perception of their personal and professional self-image.
Second victim is a term referring to the trauma experienced by staff in the wake of critical events. Where first victims are the patients and their families, second victims are the staff implicated in the event.
The term is controversial. Some argue that patients and families should not be condensed into first victims, and logically, families must be the real second victims. Staff, then, would more fittingly be third victims; or not a victim, but experiencing secondary trauma.
Steven Shorrock penned a really nice article about challenges of this term (link below).
Results
Five key themes with several sub-themes emerged in how staff coped with critical events and moving on.
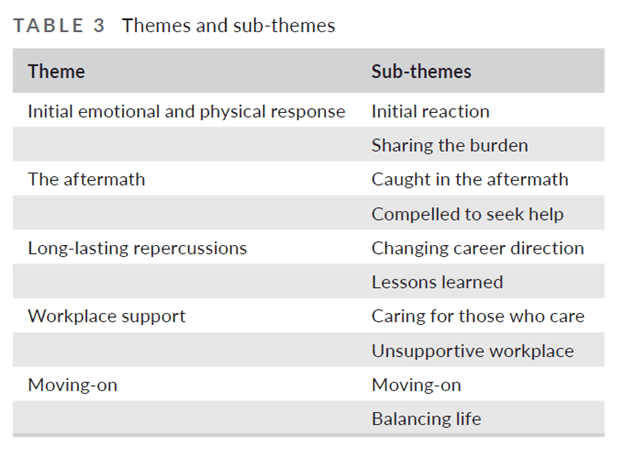
- Initial emotional and physical response
This stage involved intense emotions unleashed following critical events which left most participants “craving to share their burden with someone to reduce the impact of the event” (p6).
Key findings:
- Participants were initially left in shock at what happened, which was followed by stress and disbelief
- They relied on instincts and gut feelings to operate in autopilot to keep functioning
- Guilt and self-blame replaced initial adrenalin surge. Some felt ashamed, anger, sadness and a futility about what happened.
- Stress and guilt was fuelled by losses in professional confidence and negative thoughts
- Sharing the burden by telling the story at the initial stage helped people to be heard and understand the meaning of the experience
- Sharing the story was difficult for some people; with some being reluctant to breach confidentially and remained silent
- That is, despite the importance of talking about the circumstances, some “suffered under a veil of secrecy and in solitary silence” (p6)
2. The aftermath
This stage involved people fearing the consequences of the event, including investigations. Some people entered periods of rumination where they found ways to reduce the impact and return to work.
Job satisfaction was noticeably less for some people, and they found less enjoyment at work. Some felt they would lose their capacity for patient care and entered a state of hopelessness.
While EAP access was important for some, others saw asking for help as a sign of weakness.
3. Long-lasting repercussions
This stage involved the process people followed to rationalise their emotions associated with the event. Intrusive recollections of the events replayed in their minds, and for some this resulted in persistent insomnia and nightmares.
Some considered changing the direction of their careers or even leaving clinical care.
A degree of learning followed in this stage, where replaying the event provided an opportunity for some to amend their view of themselves, their professional practice and the workplace.
4. Workplace support
Workplace support post-event varied between workplaces. Only 2 of the 10 participants felt well cared for after the event (by way of immediate debriefing, counselling opportunities and follow-up comms from managers).
Many saw a perceived lack of managerial support for their own mental and physical well-being.
Although a “no blame culture” was in operation at most settings, 50% of participants relayed fear of being blamed for what happened.
Doubting their professionalism impacted their interpersonal relationships.
One participant lamented the so-called “no blame culture” at her workplace, saying that the only time she hears from management is when something has been done incorrectly (e.g. not signing-off a timesheet), but rarely or never a phone call saying well-done for coping with an extremely busy shift.
Another participant noted that mandatory counselling should be standard practice rather than voluntary.
Many felt the recovery and counselling procedure as “insincere because they felt their managers were simply ’ticking the box’ and left them to deal with the aftermath of the incident on their own” (p7).
5. Moving-on
This stage reflected how people balancing life and work. It was about not forgetting what happened but rather learning and coping. One participant commented that even 32 years after a critical event that she has not forgotten but has simply learned to move on.
Most participants affirmed that they have moved on from the events by using adaptive strategies. These included feeling equipped to cope (emotionally & physically), helping themselves and taking time to resolve their emotional turbulence.
For some, they focused more on themselves – like with healthier eating, exercise, meditation, more time with friends and family. For others moving on was more difficult. They had trouble maintaining their clinical role and some anticipated leaving clinical care altogether.
In wrapping up the findings, the authors noted that:
- Participants conveyed various unsupportive workplaces behaviours and responses, including a pressure that nurses were expected to just get on with work and accept it
- While some considered leaving the profession, for others they were able to thrive and learn from the event
- Personal and professional disruption experienced by second victims is “subjective and decidedly individual, thus a ’one size fits all’ discipline-specific approach must be cautioned” (p8)
- Many found telling their story to be cathartic, and in part relaying the event and their emotions with co-workers helped them receive reassurance, validation and normalisation
- The above was however challenging for many, with a fear of speaking out and therefore suffering in silence.
- To help second victims move on, this “veil of secrecy must be lifted”. This is likely more a factor of the organisation and leaders to facilitate and nurture than it is up to the individual responsibility
- On the above, while most were aware of EAP and other free counselling services, many felt reluctance to utilise it. Another study explored whom reached out first – second victims or managers, with this study founding that managers rarely ever reached out first
- Overall, organisational responses to critical events did not seem well-enough equipped to support second victims and were described as more bureaucratic back-covering exercises
Although this was focused in healthcare, the findings seem relevant to other safety-critical industries.
I noted a lot of similarities with the shame, embarrassment and guilt in construction following injuries and events – which, similarly, are focused more on other stakeholders and assets and in comparison, ill-equipped to deal with the wellbeing of the employees directly involved.
Authors: Buhlmann, M., Ewens, B., & Rashidi, A. (2022). Journal of Advanced Nursing, 2022;00:1–13.

Study link: https://doi.org/10.1111/jan.15274
Steven Shorrock’s article: https://humanisticsystems.com/2018/12/04/the-real-second-victims/
Link to the LinkedIn article: https://www.linkedin.com/pulse/moving-after-critical-incidents-health-care-study-ben-hutchinson

One thought on “Moving on after critical incidents in health care – A qualitative study of the perspectives and experiences of second victims”