This study explored the question “where do Resilience Skills (RS) come from?” by way of interviews, questionnaires, observations & document analysis in two emergency departments.
RS are defined as “skills of any type necessary to adjust performance, in order to maintain safe and efficient operations during both expected and unexpected situations”. Studying RS is said to be important due to healthcare systems being widely regarded as primary examples of complex systems.
RS are evaluated from the perspective of Resilience Engineering and incorporated evaluations of work constraints & other factors. RS have been likened to similar constructs like non-technical skills.
Results
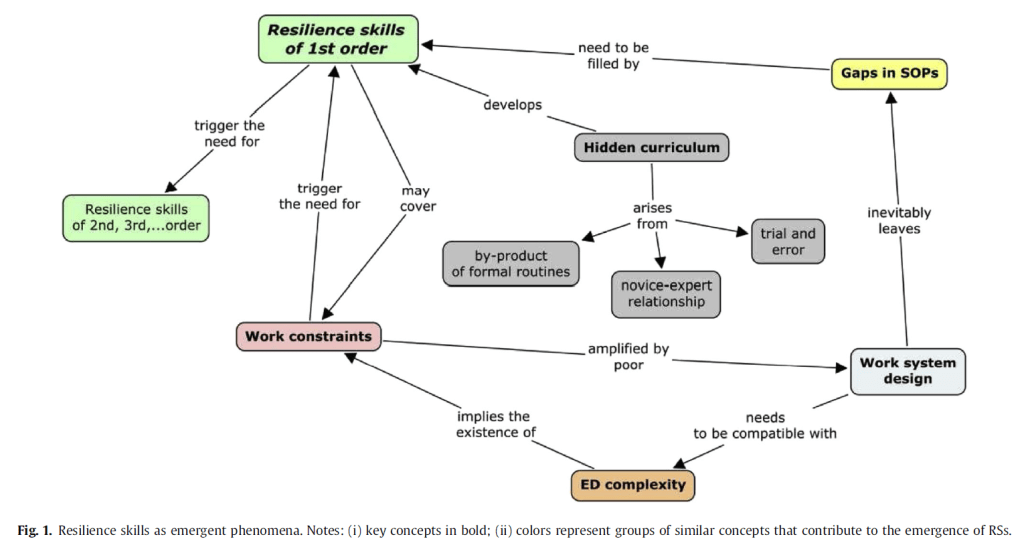
Overall, individual RS arise from the interactions between work constraints, hidden curriculum, gaps in SOPs, org support for resilience, and RS themselves. The use of RS “occurs on an everyday basis by ‘normal people” (p235), and don’t require extraordinary actions by outstanding performers.
A range of RS were identified. Collaborative work was the most cited skill, and is characterised by team problem solving and sharing responsibilities.
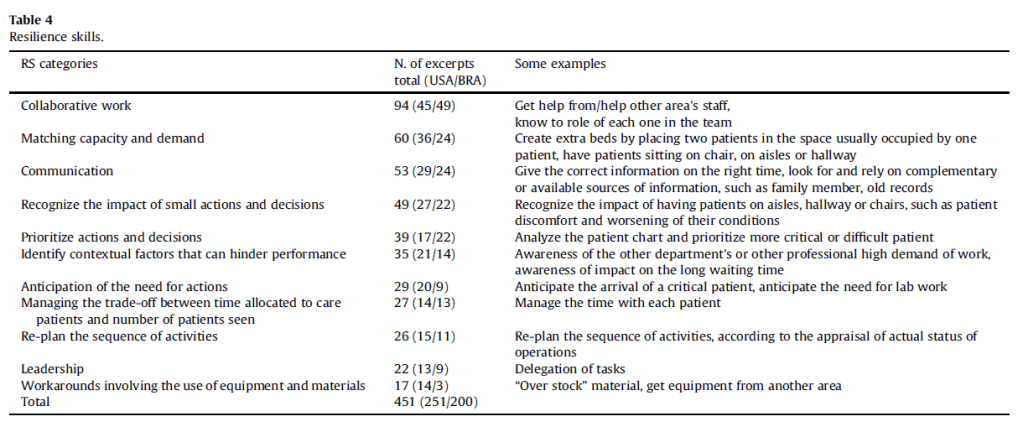
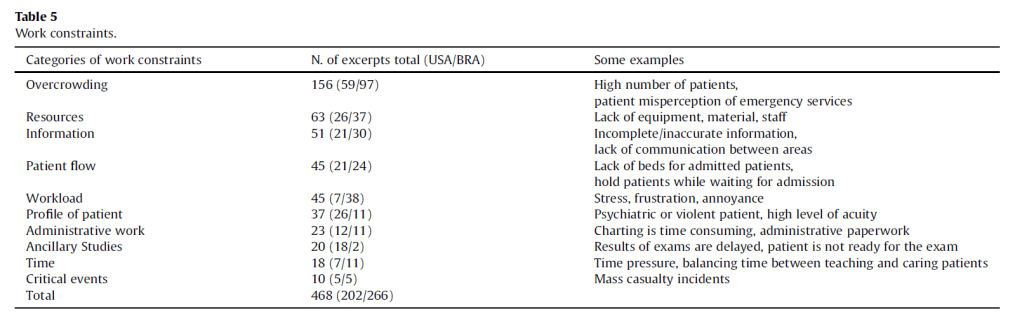
Matching capacity with demand was the second most used RS. This was largely a result of overcrowding wards and variability of demand.
Of interest, no RS was devoted solely to learning, which “may indicate both a weakness of both [emergency departments] as well as that learning emerges from the joint use of several RSs” (p230).
The responsibilities for resilient skills don’t rely solely on frontline staff – data between the emergency departments suggests that the degree of organisational resources and support for these skills varies substantially. Greater support may encourage the development of RS, as professionals “increase their repertoire of work strategies” (p232).
However, importantly, evidence also suggested that work constraints triggered the use of RS, such as responding to overcrowding or matching capacity to demand. It’s suggested that the variety and intensity of work constraints can act as a proxy measure for the complexity of the work situation, and thus of the need for RS. Thus, a lack of resources or appropriate support may also facilitate RS to cope with these issues.
Another consideration was around hidden curriculum (HC), which is the unplanned learning that occurs during everyday practice from trial & error. Skills from HC are not explicitly taught in classes or seminars. This included how experienced healthcare staff prioritised which patient gets medicated first. HC can facilitate the learning of some RS.
However, a downside of HC is that it may “perpetuate ineffective workarounds that are (wrongly) taken for granted” (p233).
Indeed, RS are sometimes used more frequently than necessary – and therefore, RS which develop as a result of the environment may conceal underlying system deficiencies, and perpetuate a feedback loop requiring more resilient skills to cope. This process may only stop when the “system runs out of adaptive capacity and stops producing outputs” (p234).
As said by the authors, RS are recursive: resilience demands more resilience. This may not address underlying system issues.
Finally, they provide advice on how to utilise RS to develop training programs. For instance, it was possible to identify emergency department operations likely to have gaps – and thus require RS to fill the gap.
Therefore, targeted training and development of appropriate RS would be useful.
Authors: Wachs, P., Saurin, T. A., Righi, A. W., & Wears, R. L. (2016). Applied ergonomics, 56, 227-237.
Study link: https://doi.org/10.1016/j.apergo.2016.02.012
Link to the LinkedIn article: https://www.linkedin.com/pulse/resilience-skills-emergent-phenomena-study-emergency-ben-hutchinson

One thought on “Resilience skills as emergent phenomena: A study of emergency departments in Brazil and the United States”