An interesting study exploring workplace adaptations at all stages of the vein to vein blood transfusion.
Although transfusion is considered one of the safer areas of healthcare, some deaths are still associated with transfusions each year. An earlier study from these authors found a tendency for individual staff members to be blamed for incidents, rather than a search for system-related factors.
Transfusion was explored in three UK hospitals. 66 adaptations were identified from 37 participants.
I couldn’t cover all of the key points.
Results:
Overall, it was found that adaptations were “often forced upon the employees by unforeseen issues” (p502). 83% of adaptations were forced, reflecting situations where coping strategies are required rather than being able to implement ideal solutions.
The two largest triggers requiring staff to adapt were staff-related issues and poorly designed health IT systems, that couldn’t be amended or redesigned quick enough.
For staff issues, it related to things like lack of staff, employment of less qualified staff, or where less experienced staff impacts on more experienced staff who adjust for the limitations.
An example of adapting to staff experience was one ward requesting all blood components to be irradiated (an over-specification and waste of resources), because of lack of experienced staff to know when to specifically request irradiated components. This adaptation also demonstrated ETTO (Efficiency-Thoroughness Trade-Off), where thoroughness is emphasised to mitigate risk of less experienced staff.
Other adaptations involved compensating for facility problems (e.g. poor A/C temperature regulation in the lab), adoption of cost-effective technology solutions (using a baby monitor for communication between staff), and interim process changes while awaiting IT amendment and temporary local adaptions (phoning patients for more information; using personal stamps for envelopes to speed up letter delivery).
Adaptations were more likely to occur in a different part of the system to the adaptation’s trigger (70% different part); that is, unable to resolve the source of the issue and thus make changes elsewhere. This highlights how adaptations tend to be carried out within the staff members’ sphere of influence, rather than addressing the underlying management or technological issues – seen to be out of their control.
Where adaptations did occur, it was principally the process that was amended, or changes to a specific task were made.
Here, authors note that changing “a different part of the system may be a less desirable adaptation, but not necessarily less resilient” (p501). Nevertheless, adaptations aren’t always the most ideal even when focused on the same area as the trigger because of wider issues like resource constraints.
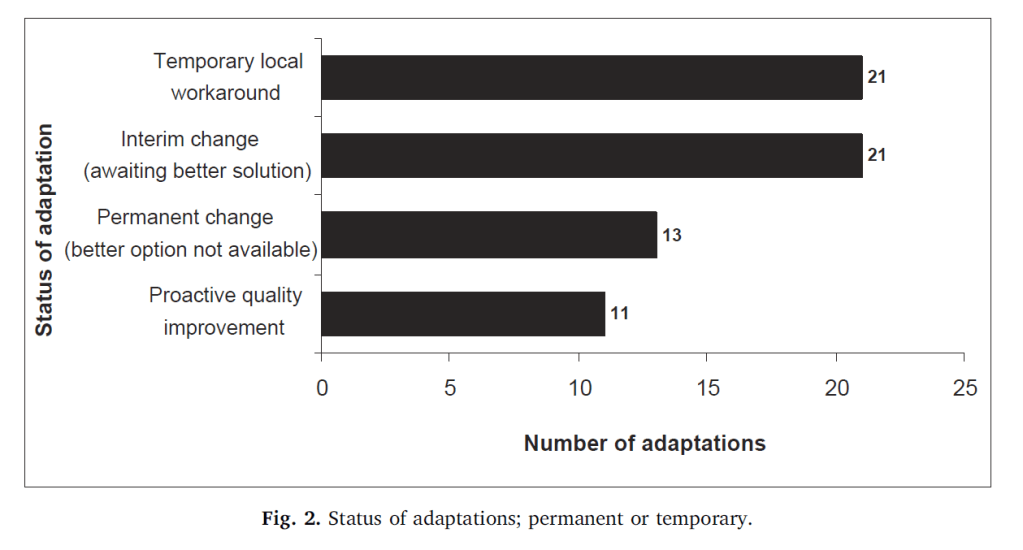
Also analysed was the permanency of adaptations. A minority were deliberate system/process quality improvements (17%), compared to 20% which were permanent but forced adaptations (ideal solution not going to be available in foreseeable future). Most adaptations were provisional and interim, waiting on a more ideal solution.
Interestingly, in 80% of the responses it was revealed that managers/colleagues were unaware of the adaptations made. Thus, adaptations were “commonly made without the involvement of management or departmental colleagues” (p502). These find and fix approaches may discourage reporting and better organisational learning of problems.
Forced adaptations were said to show system deficiencies but reveal how staff felt the need to adapt. Therefore, adaptations may be “valuable indicators at a local level of a system that is liable to fail, i.e. a potential future accident/incident could be prevented” (p503); e.g. as an indicator of brittleness. Understanding these factors is critical, since “trade-offs are made to accommodate sustained resource pressure, so organisational resource constraints can potentially magnify exposure to risk” (p501).
Further, authors highlight the problem with blaming individuals for amending process/procedures, as “that amendment might have previously been necessary and successful on numerous occasions” (p504).
Thus, understanding how to assess the nature of adaptations could help improve the safety of healthcare systems, rather than concentrating on improving the resilient potential of individuals within the system.
The temporary status of the workarounds are shown below:
Authors: Watt, A., Jun, G. T., & Waterson, P. (2019). Resilience in the blood transfusion process: Everyday and long-term adaptations to ‘normal’work. Safety Science, 120, 498-506.
Study Link: https://doi.org/10.1016/j.ssci.2019.07.028
Link to the LinkedIn post: https://www.linkedin.com/pulse/resilience-blood-transfusion-process-everyday-normal-work-hutchinson

One thought on “Resilience in the blood transfusion process: Everyday and long-term adaptations to ‘normal’ work”