This systematic review evaluated whether Root Cause Analysis (RCA) is an adequate method to help decrease the recurrence of avoidable adverse events (AAE) in healthcare.
21 studies (from an initial pool of 127) met inclusion requirements.
Results:
Overall, this study found that “Although early studies suggested that RCAs are effective in promoting ideas for preventing recurrence, more recent studies do not confirm these findings” (p12, emphasis added), and based on available evidence, RCA “does not seem to produce enough benefits to address the problem … and thus, avoid possible AAEs” (p11, emphasis added).
In only two of the studies could it be established that RCAs contributed to improvement of patient care to some extent; but both studies were limited by the total number of RCAs reviewed. In 50% of reviewed cases, the recommendations made were weak & didn’t lead to a reduction of AAEs.
A common gap limiting the effectiveness of RCA seems to be that they’re not usually coupled with verification of whether the devised improvement plan is carried out. Further, other research warned that poorly designed action plans and measures may “generate new risks and may be insufficient to prevent the occurrence of new events” (p8).
One study found that the action plans often didn’t follow any pattern of controlled implementation; and thus, authors couldn’t establish any link between the action plans on AAEs.
Found was that in many RCA recommendations, latent conditions were neglected in favour of focusing on active errors of operators. It’s said that describing events from a perspective different from individual error is challenging for professionals – who are sometimes reluctant to participate because of distrust generated by possible future consequences (blame). [I’d add that many RCA frameworks provide little guidance for practitioners to think systemically also.]
Further, a lack of trust and a belief “that the culture is focused on the search for those responsible, in addition to creating tension in the work environment that may cause interprofessional problems … is one of the main reasons for professionals refusing to participate in incident reporting systems” (p9).
Also found was that managers & personnel involved in the actual AAEs had low participation in the investigation teams. Besides limiting their unique knowledge & insights [of WAD], this also limits positive effects of recoveries of second victims by limiting their involvement in solutions.
Although the authors are charitable in saying that RCAs appear to have “considerable validity” in learning about incidents, they conclude that the recommendations resulting from RCAs “were not useful enough to prevent the same incidents from recurring in the future” (p11, emphasis added).
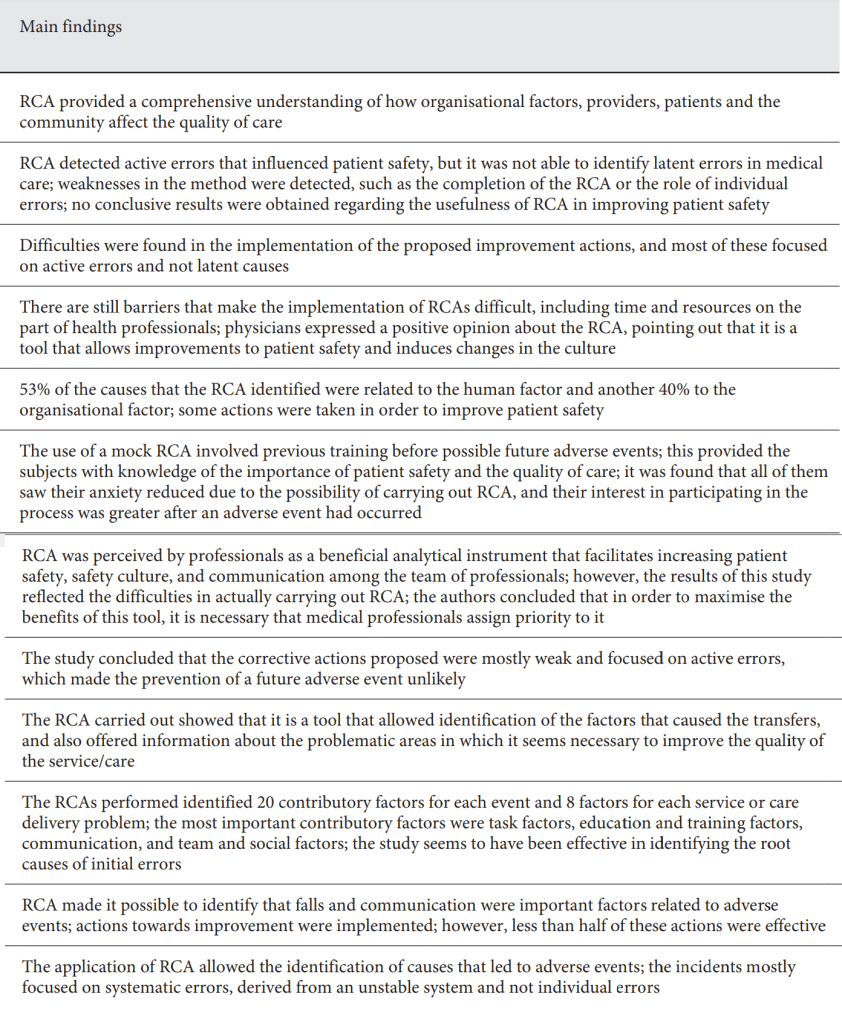
Nevertheless, this isn’t to say that there isn’t value in undertaking these types of investigations and reviews – see below for some of the main findings from the included studies:
Authors: Martin-Delgado J.a · Martínez-García A.b · Aranaz J.M.c · Valencia-Martín J.L.c · Mira J.J, 2020, Medical Principles and Practices
Study link: https://doi.org/10.1159/000508677
Link to the LinkedIn post: https://www.linkedin.com/pulse/how-much-root-cause-analysis-translates-improve-ben-hutchinson

One thought on “How much of Root Cause Analysis translates to improve patient safety: A systematic review”