Thought this attached guidance on developing checklists may be of interest
(Of course, books, journal volumes, and careers revolve around checklist development.)
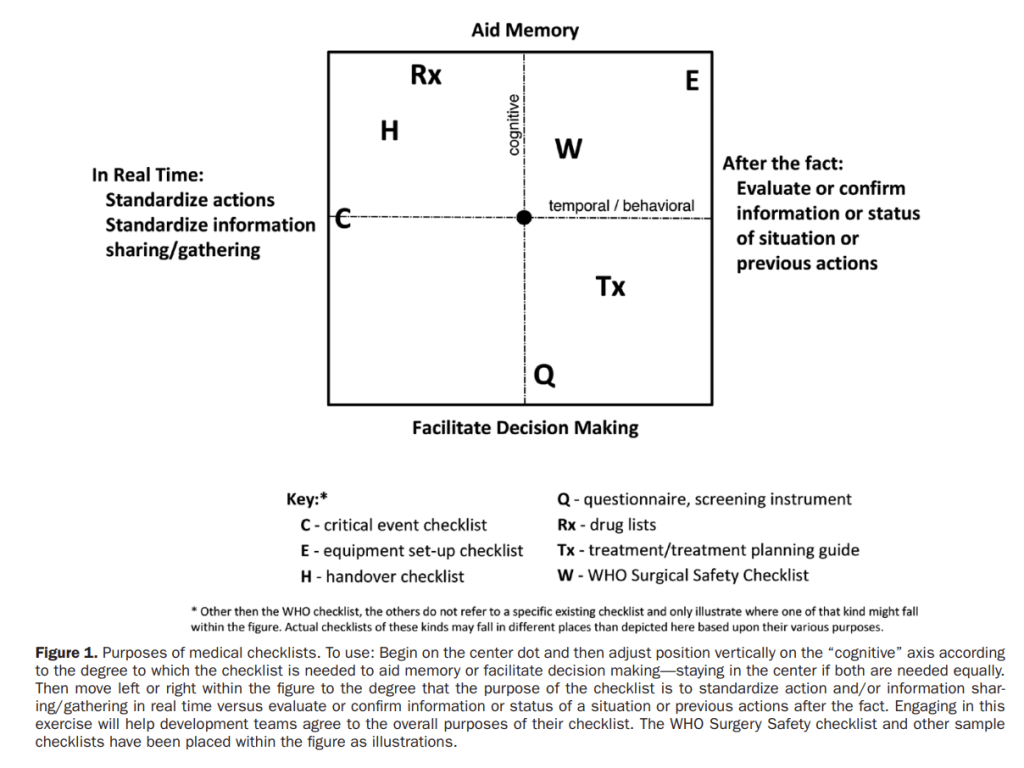
For healthcare checklists, they offer image 1.
Based on a previous systematic review of literature – just 7 articles out of 91 mentioned issues with the conception of a checklist. That is, asking whether a checklist is actually the most appropriate intervention.
Next, according to image 1 – designers should not just jump into writing down items for the checklist, but start by “thoroughly exploring the checklist’s purpose and desired outcomes”. Is the checklist designed as a memory aid or to facilitate decision making – or both?
They also highlight that:
1) “A checklist that simply appears with no introduction, training, or rationale as to why it is needed is unlikely to be accepted”
2) “Training using standard, predictable, or “textbook” scenarios is not sufficient to ensure effective use across all situations”
3) Thus, training should involve some sorts of scenarios before used in real practice. Scenarios should include more complex yet realistic perturbations and combinations of conditions (e.g. how people use checklists, in what conditions, and where do they start on the checklist – at the start or at some other point mid-way?)
3a) [On the above, perturbation-based training can be really useful, as we typically train people based on standard conditions rather than problem-solving and building capacity during fault finding and out-of-basis events]
4) Observations of physicians found that they often do not follow checklists in a linear manner, e.g. starting at the top and working down
5) “Instead, many first use existing knowledge and refer to a checklist for additional ideas or specific information (eg, drug dosages) only after starting treatment”
6) Further, “Checklists designed for use in a stepwise fashion generally do not support this kind of specific information-seeking behavior. Checklists for medicine that too closely follow an aviation-oriented design may therefore be ineffective”
7) High-fidelity simulations can be useful but not necessary. Low-fidelity simulations can also be effective – particularly if people are asked to verbalise and expand on their decisions along key points
8) They note that, “the science of how to do checklists is in its infancy.”
9) “checklists do not work in isolation; they are part of a complicated, dynamic, sociotechnical system … and many cultural and systemic changes are also necessary for checklists to achieve their potential”
This work is supported by other work which suggested checklists are used as ‘resources for action’.
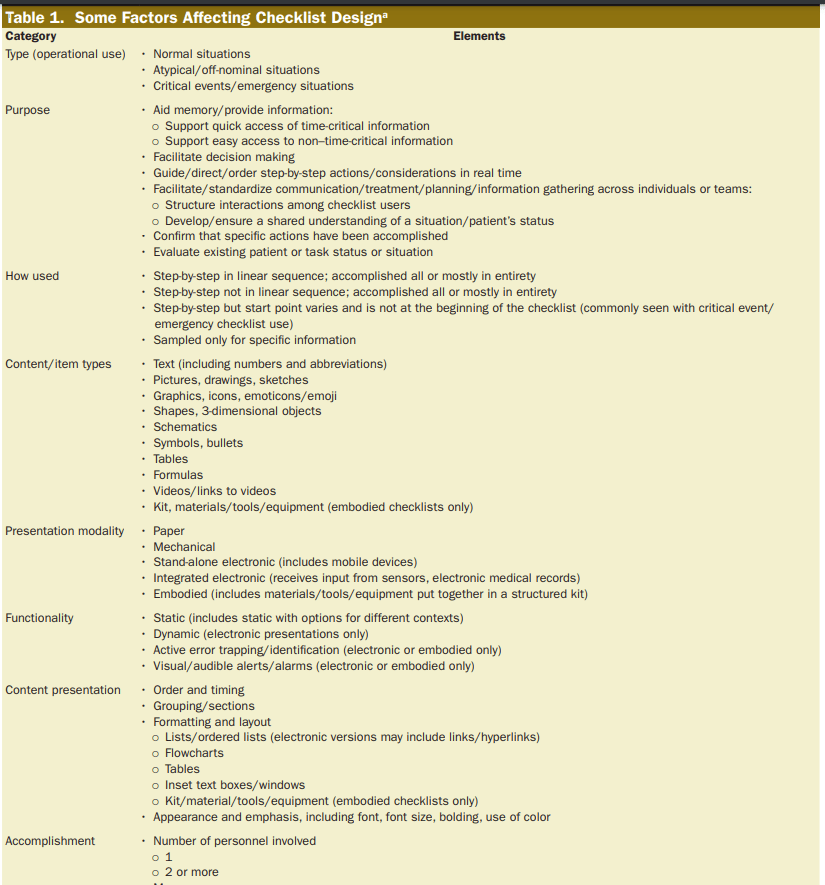
Image 2 covers some factors influencing checklist design.
Ref: Burian, B. K., Clebone, A., Dismukes, K., & Ruskin, K. J. (2018). Anesthesia & Analgesia, 126(1), 223-232.

One thought on “Checklist design”