Do different near miss types result in different organisational learning responses?
A 2021 paper I summarised, with Amy Edmondson as co-author, explored this question. Post in the next couple of weeks.
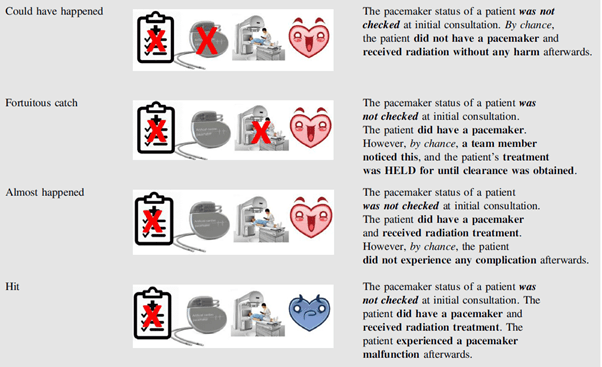
The six event types were:
- Hit: adverse events resulting in patient harm.
- Potential hit: events that reach the patient, but do not result in immediate harm (but may manifest in harm later on).
- Almost happened: near misses that reach the patient, but no harm results. They note “In retrospect, these events contain prior signaling of potential harm (eg, the presence of a pacemaker), that is, the enabling condition for harm, as well as a latent error by staff (eg, not checking the pacemaker status)” (p258).
- Fortuitous catch: Also called a good catch, these are events that don’t reach the patient and are averted by chance from human intervention.
- Could have happened: near misses that don’t reach the patient and don’t contain prior signals of the enabling conditions. E.g. the pacemaker status wasn’t checked prior to radiation, but the patient didn’t have a pacemaker anyway. These types are said to contain only active conditions (rather than latent).
- Process-based catch: near misses that are averted by a systems-based process or check for the enabling conditions. E.g. the process requires staff to check for pacemaker status and the staff correspondingly check for the pacemaker.
They found that “could have” events were viewed as “less successful” than “almost happened” events, and more likely to be reported as learning events.
Fortuitous catches were seen as more successful – even though they had the same enabling conditions as more severe event possibilities. However, people were more likely to report them, probably because they were seen as examples of “system resilience”, and thus, probably less fear of reporting these.
They also note that there could be false confidence in relying on safety processes if those processes are inefficient or not adhered to [* no surprises here of course.] Hence, organisations must better engage from workers and learn from normal situated work to remove “deadweight” processes and decentralised problem-solving mechanisms.
Ref: Kundu, P., Jung, O. S., Valle, L. F., Edmondson, A. C., Agazaryan, N., Hegde, J., … & Raldow, A. (2021). Practical Radiation Oncology, 11(3), e256-e262.
Other studies on near miss/near hit learning:
a) https://www.linkedin.com/posts/benhutchinson2_how-to-avoid-catastrophe-activity-6892592292524376064-RSbc?utm_source=share&utm_medium=member_desktop
b) https://www.linkedin.com/pulse/new-ways-learn-from-challenger-disaster-almost-30-years-hutchinson
c) https://www.linkedin.com/pulse/airline-safety-improvement-through-experience-tale-ben-hutchinson
https://www.linkedin.com/pulse/near-miss-events-risk-messages-decision-making-ben-hutchinson
d) https://www.linkedin.com/pulse/research-bite-how-near-misses-influence-decision-under-ben-hutchinson/

One thought on “Near misses and good catches and their relationships to learning, or not”