This reviewed the published evidence for the interventions and measurements used in HRO implementations (and lesser degree, RE).
Of 1400 studies 34 were included. Given overlaps with resilient organisation and RE concepts, some of this work was also included.
A key focus was on the question “how do you know if you’re an HRO and how do you validate it?”. Way too much to cover, so I’ll pick a few themes.
Note: I’ve also posted studies exploring the links between HRO and performance, so check out my site if you’re interested.
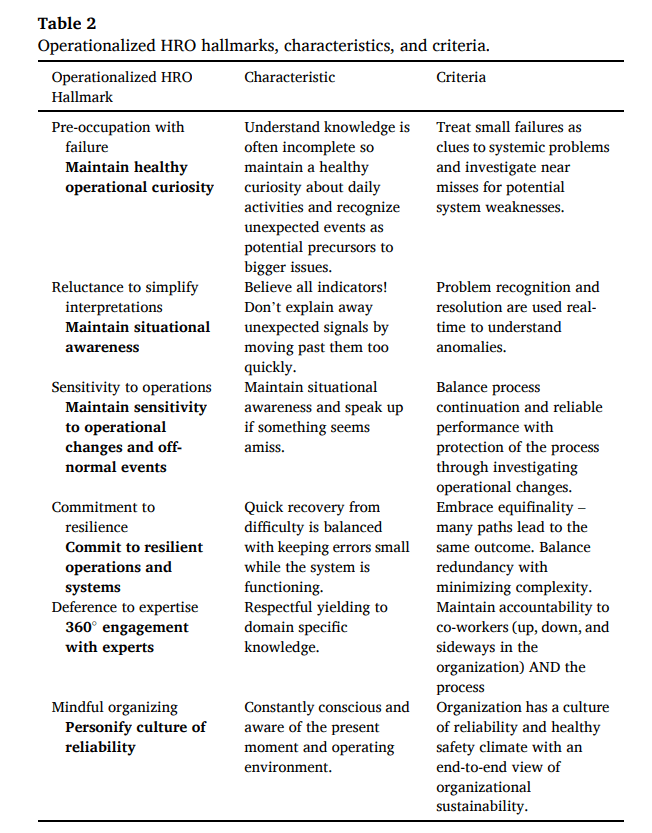
Below is a snapshot of key HRO hallmarks:
Results
The review indicated that while HRO has spread into virtually every sector there are still no published prescriptions on implementation. One study noted that operating as a HRO may be “as simple as applying standard Industrial Engineering and business tools with a focus on HRO characteristics”, whereas other work, after reviewing emergency room resilience literature, found a lack of investigation on the technical tools to support individuals and firms toward achieving resilient performance.
This led the current authors to question whether HRO is perhaps easy to conceptually understand but harder to quantify and apply.
Overall, 3 key themes emerged from HRO implementation:
1. Process redesign (workflow analysis, new models and frameworks, checklists, error reporting systems). Process redesign interventions were the most diverse theme and also included coaching ‘mindfulness’ practices. Traditional process improvement tools like six sigma, lean and process mapping were suggested as useful for implementing HRO practices.
2. Organisational redesign (creating ad hoc and multidisciplinary teams, structural changes). This typically focused on improving cultural/climatic factors or improving specific underperforming groups.
3. Training interventions (focused around simulations or training employees on HRO).
Against Weick and Sutcliffe’s 5 HRO hallmarks (1 Preoccupation with failure, 2 Reluctance to simplify, 3 Sensitivity to operations, 4 Commitment to resilience, 5 Deference to expertise), pre-occupation with failure and reluctance to simplify were the most common in health care, whereas pre-occupation was more common in non-health care.
Despite the hallmarks having significant overlap, preoccupation with failure is more often implemented as a measurable intervention across all sectors. Authors reason this may be because since HRO/RE focus on the ability to detect, adapt and evolve to manage performance, it makes sense that firms will focus on instances that disrupt performance.
For implementation of HRO reform, no study mentioned that improvement in any specific hallmark was sought but rather firms were aiming to become more like a HRO overall. That is, most firms adopted HRO practices and measured metrics relevant to their industry rather than measuring the presence of HRO itself.
Only two firms mentioned their HRO change as part of a structured plan.
Higher frequency of preoccupation and sensitivity to ops suggested that firms explored strong responses to weak signals as a means of improving organisational outcomes – while then realising sensitivity should be included.
Across all firms, commitment to resilience was the least implemented, despite a multitude of tools to measure facets of capacity for resilience. This may be due to relying on understanding organisational systems through process mapping and understanding work, thus potentially requiring an enormous undertaking.
Further, studying redundancy, slack and flexibility may also be laborious for many firms.
As noted here and elsewhere, there’s no single [capacity for] resilience metric and firms must adapt their own metrics to establish if various aspects of resilient capacity are present, increasing or decreasing.
Whereas other hallmarks were attempted in relative isolation of each other, reluctance to simplify was only used as an intervention in combination with other hallmarks. Reasons are unclear but authors posit that maybe it’s less understood or maybe it can’t be attempted in isolation.
Some research argued that both HRO and RE researchers “failed to publish specific safety enhancing strategies for various parts of a single, or system of organizations” (p6). Other argued the difficulty of even separating HRO interventions from other concurrent ones such that it’s hard to know if improvement is attributable to HRO practices or not.
Overall, authors conclude that “three specific interventions have been used which were useful and generalizable to guide practitioners in moving toward an HRO state: process redesign, training, and organization redesign” (p1) and that “We suggest that this evidence may assert that organizations which are not functioning as an HRO can be redesigned to do so” (p1).
Authors note that capacity for resilience is integral to organisational sustainability and that it goes beyond component reliability, multiple controls, redundant systems and simple operational alternatives, where “the fundamental element of successful resilience is people, and the redesign of organizational systems, processes, and interfaces should focus on facilitating the re-engineering around human factors, rather than the mechanistic, inorganic ones.” (p6).
However as per other lit reviews, research is “highly focused on theoretical discussion and only lightly focused on interventions to implement high reliability” (p5); making it hard to draw clear conclusions.
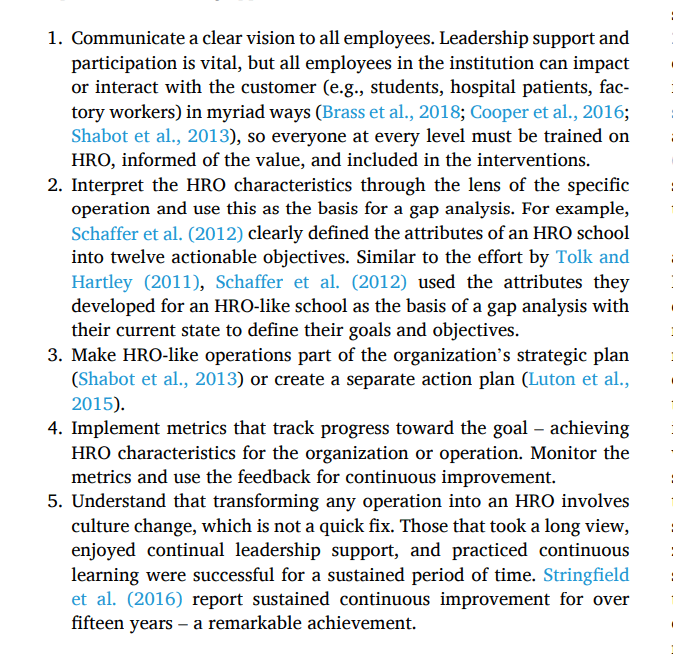
All of the studied organisations which successfully employed HRO principles seemed to have used the following approach:
Authors: Cantu, J., Tolk, J., Fritts, S., & Gharehyakheh, A. (2021). Applied Ergonomics, 90, 103241.
Link: https://doi.org/10.1016/j.apergo.2020.103241
LinkedIn post: https://www.linkedin.com/pulse/interventions-measurements-highly-reliableresilient-ben-hutchinson-b6iuc
