This study analysed 75 investigation reports from the U.S. Chemical Safety and Hazard Investigation Board (CSB).
The authors coded the reports based on attributed causal/contributory factors and the types of corrective actions assigned.
Providing background:
- They argue that many investigations only provide general knowledge to the Chemical Process Industry (CPI) instead of “understanding and implementing efficiently the adequate accident corrective measures”
- One study found that “only one third of accident cases are considered to provide lesson learned on a broader basis” and that “most accident reports are not informative and beneficial enough to CPI players in terms of learning from previous accidents”
- Other research looking at the learning cycle following incidents argued that the “current cycle of learning system is not sufficient enough in preventing accident occurrence due to poor input quality, lack of analysis, poor dissemination and insufficient use of information”
- Further, it’s reasoned that the “weakest link” in the learning cycle is information dissemination, as “as majority of research on experience feedback only related to accident investigation and not much on information dissemination”
- The authors then talk about different options for organisations, like management system or engineering controls. Then they talked about Layers of Protection (LOP)
- LOP can be classified into four categories in decreasing order of reliability: inherently safer (IS), passive engineered, active engineered and procedural safety
- IS eliminates hazards, while passive engineering uses process and equipment design to minimise hazards; both are more reliable since they depend on physical and chemical properties of the system rather than “successful operation of instruments, devices, procedures and people”
- Active engineered controls, like interlocks, emergency shutdown systems etc. rely on technology to identify and respond to process deviations, whereas procedural processes rely on people
- IS and passive engineering can be considered as ‘strategic approaches’ best implemented early in the design lifecycle, whereas tactical approaches, like active engineering and procedural, tend to be implemented later in the design life
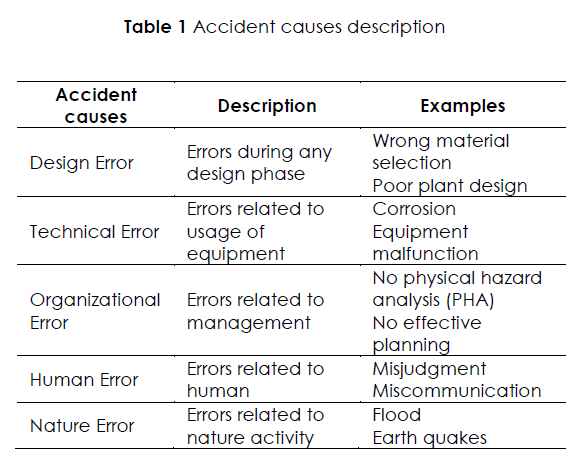
In this study, they grouped the accident factors into errors…for some reason. Of course, these types of categories depend on worldview, definitions etc, and are more indicative of the analysts, so I suggest you don’t take them too literally.
If you get stuck on the error term then do what I did and replace it with ‘factor’ and move on with your life.
More interesting I think are the types of corrective actions employed by organisations in response to the findings.
But anyway here they are:
Results
They found:
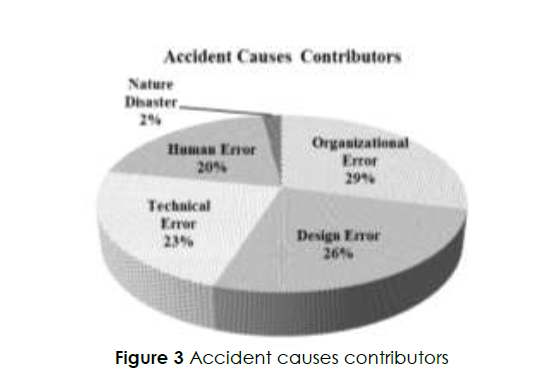
- Organisational factors was the highest contributor at 29%
- Design was the second most frequent contributor at 26%, technical error third at 23%, and human error at 20%, and natural disaster at 2%
Human and organisational factors was reflected in things like lack of process hazard analysis and no effective planning. Design was mostly related to wrong material selection, inadequate detection and protections and inadequate HAZID during design phase.
Technical errors were reflected in factors like lack of supervision [** which seems odd for a technical factor?] and poor documentation. Human performance factors were related to things like inadequate knowledge and training, miscommunication and unintended actions.
Prior data from Lees related 47% of chemical accident factors to organisational factors, 29% to technical factors, 16% to human performance, and 8% to design factors.
Newer data has related 79% of chemical accident factors to design issues, with the remaining from human and organisational factors during operation stage and external factors.
Data is summarised below:
For corrective actions – procedural actions were not surprisingly the most frequently assigned actions.
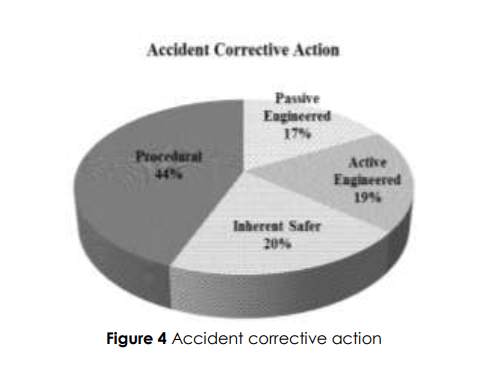
IS made up 20% of actions, 19% for active engineering, and 17% for passive engineered.
The authors highlight the mismatch between accident contributors and the hierarchy of corrective actions, such that “the contribution of design and technical errors to accident is significant i.e. 49%, however majority of the corrective action taken are based on procedural (44%) strategy”.
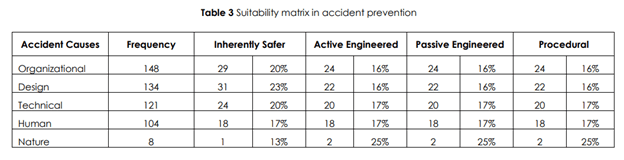
That is, design and technical problems should ideally be addressed with engineering rather than procedural. Not surprisingly, procedural actions were the most common response for all types of accident contributors.
Another finding based on this sample was that chemical accidents seem to “recur every 5 year interval”. Moreover, in 58 cases of accidents, 26 cases (32%) reoccur within the same company, while 32 cases (39) happen in similar operations in different companies.
They note that “Only 29% accidents are caused by unique causes”.
Finally, they report that a “Large majority of the recommendation are made without proper investigation and risk analyses. Therefore, less reliable and easy to implement corrective actions were recommended without considering design changes and engineered add-on safety measures.”
Because of this weak approach, “the hazard still in the process and the likelihood of accident is high due to fragile safety barrier chosen”, and the organisation “usually overlooked the need for hazard identification process because they are happy with the current safety performance and focusing on routine daily operation issues”.
Some organisations were said to lack a system to continuously identify and monitor process and personal hazards in the workplace.
See below for a breakdown of which types of improvements were used for each level of contributory factor:
Authors: Jalani, J. A., Kidam, K., Shahlan, S. S., Kamarden, H., Hassan, O., & Hashim, H. (2015). An analysis of major accident in the US chemical safety board (CSB) database. Jurnal Teknologi, 75(6).
Study link: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=dbf85b55d0e079f3ee842ba78529d8a5e1746f2d
LinkedIn post: https://www.linkedin.com/pulse/analysis-major-accident-us-chemical-safety-board-csb-ben-hutchinson-7eekc

One thought on “An analysis of major accident in the US Chemical Safety Board (CSB) Database”