This coroner’s report detailed the sad case of a medical misdiagnosis, resulting in a death.
Here, a young adult died due to undiagnosed bacterial meningitis, diagnosed primarily as middle ear infection (the ear infection led to meningitis).
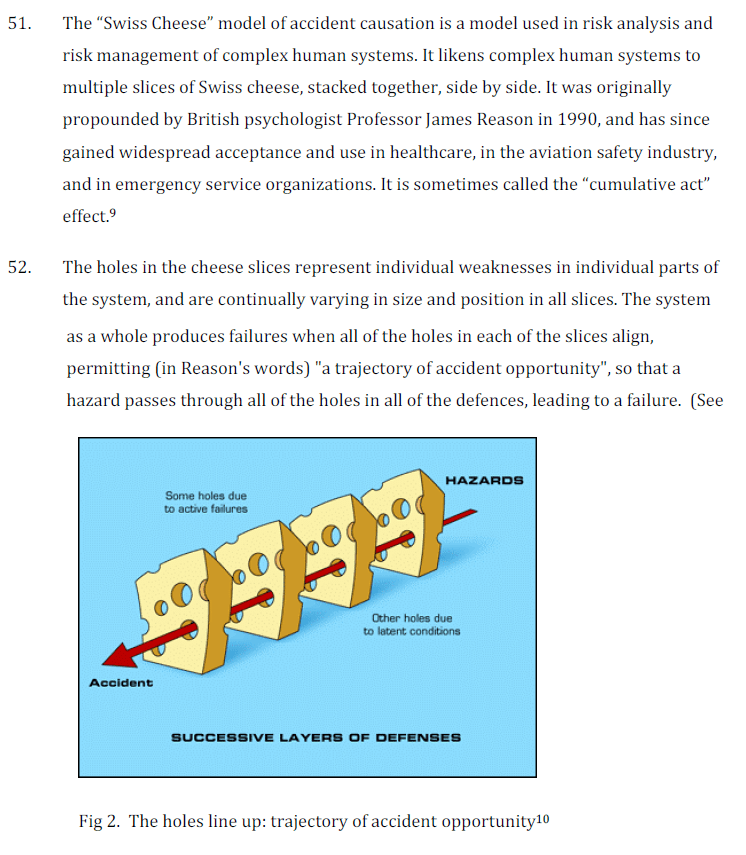
Interestingly, the coroner framed the core findings using the Swiss Cheese metaphor (** despite its limitations in complex systems and interactions vs. AcciMap, STAMP, Rasmussen’s dynamic risk etc., it holds up OK for a general lens and isn’t as linear as some say).
Describing the event:
· Drs are trained in medical school to think via “differential diagnoses” and to exclude the most serious illnesses before diagnosing. This is usually accurate enough [* satisficing], but impacted by factors like availability bias – judging likelihood of an event by how easily examples come to mind
· Here, the Dr quickly established a diagnosis of otitis media and “Everything she thought she saw in this clinical picture tended to confirm this impression”
· However, the Dr excluded other factors that didn’t fit the picture. The Dr “went on to make the mistake that has been described as “anchoring” – she did not consider the multiple possibilities the signs and symptoms suggested”
· Fatigue may have been a factor in the misdiagnosis. Research indicates that the decisions a clinician makes early in the shift can be different from those later in the shift, where later on there’s a greater tendency to use “intellectual shortcuts”
· Overall, “The ability of one individual to succeed in high-density decision-making is finite”
· Greater saliency was given to the feedback from caretakers (nurses and the like), rather than from the patient and family
· Experience of physicians was also a possible factor. The “mental menus of differential diagnoses are likely to be considerably slimmer” for junior physicians compared to senior physicians, where the patient, in hindsight, didn’t have enough oversight from a more experienced physician
· The coroner discusses the role and utility of in-house protocols, guidelines and checklists etc.
· Here it’s said “It is well-known, however, that in any complex organisation, voluminous guidelines and protocols tend to sit unread in large folders or on organisational intranet servers, rarely referenced unless something goes wrong”
· It is “unrealistic to think that doctors working long hours in very busy Emergency Departments will often have time to make close studies of large, complex documents during their shifts”
· However, there is still a place for checklists or short guidelines to act as “aides memoire, especially for less experienced practitioners, to prompt memory and thinking about certain types of problems or to ensure that patients are investigated correctly and that their treatment is carried out in the correct sequence”
Ref: Local Court of NSW. Inquest into the death of Michelle McIlquham, 2012.
Report link: https://coroners.nsw.gov.au/documents/findings/2012/michelle_mcilquham_findings.pdf

One thought on “Coroners report on fatal medical misdiagnosis: availability bias, anchoring, fatigue and “voluminous guidelines” that sit unread”