This study evaluated the impact of an integrated Crew Resource Management (CRM) training program on failure to rescue (FTR) mortality.
Two hospitals, one control and one intervention, were compared after 3 years. The CRM program in the intervention hospital consisted of a 4-hr comprehensive CRM program and included all surgical services employees (>1,600 people), and >10,000 patients.
FTR is an outcome measure describing a clinician’s inability to save a hospitalised patient’s life after experiencing a complication that wasn’t present on their admission.
I expect some will be critical of whether a CRM program should or would correlate with FTR mortalities (given their complex nature), and rather rare nature (compared to non-fatal outcomes). From what I can tell, the CRM was just a single 4-hr training session (coupled within a larger program).
Providing background:
· Other work has suggested that CRM training can improve patient outcomes in healthcare, but its effects on FTR is unknown
· Some work found that CRM improved staff outcomes but did not improve patient outcomes as expected; perhaps suggesting CRM is best used to target changes in staff behaviour and staff outcomes
· Hence, CRM approaches may not be as effective for fatal events or patient safety outcomes since these events involve intricate, multifaceted influences
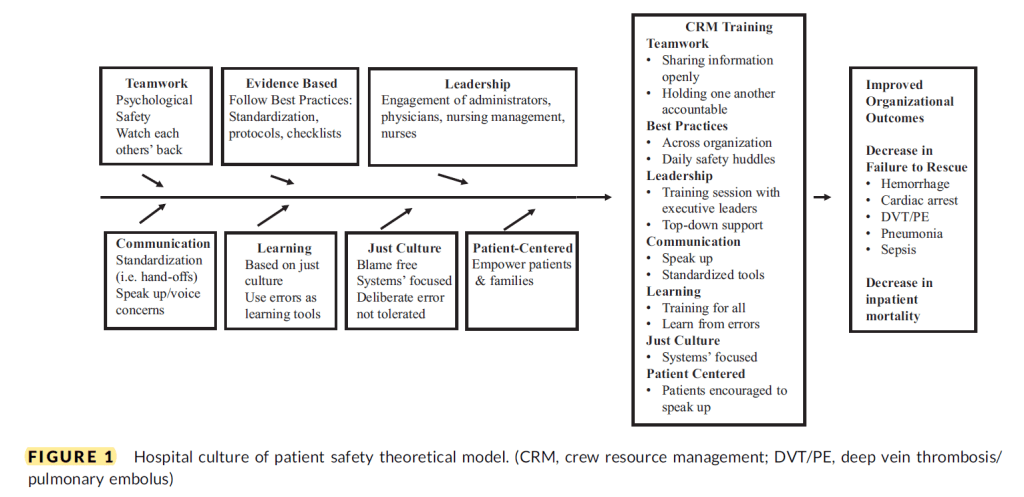
· CRM emphases six key areas: Managing fatigue, creating and managing teams, recognizing adverse situations and red flags, cross-checking and communication, decision making, and performance feedback
· They say that team members learn to cross-check each other’s actions and address errors (performance variability) in a non-judgemental way. They also undertake debriefing activities and providing feedback
· CRM have shown some promise on staff outcomes, like improved perception of the patient safety climate, improved health team member attitudes towards fatigue management, team building, comms, team decision making, adopting rules of conduct for expected staff behaviour in operating rooms and more
· Some findings of CRM in patient safety are mixed. Several studies found improvements, whereas other work found no improvements on measured indices
Results
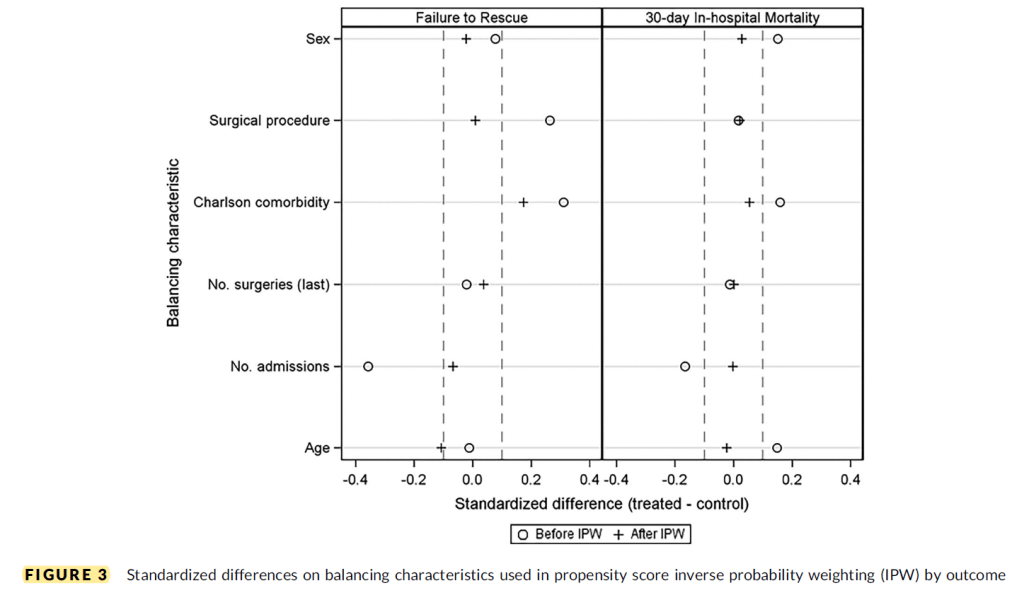
Whereas the researchers hypothesised that the CRM-trained intervention hospital would have led to improvements in teamwork, comms and other CRM-related factors, which would subsequently bolster the prevention and mitigation of OR errors (e.g. during surgery, or picking up on problems postoperatively more quickly), no significant difference was found on the probability of FTR or in-hospital mortality (after controlling for volume).
While higher mortality rates were found at the intervention hospital versus control, this wasn’t statistically significant.
They conject why these results occurred. For instance, perhaps “CRM training is best used to target changes in staff behaviors and improvement in staff outcomes rather than patient-related outcomes”.
Moreover, it’s possible that “reductions in FTR and IM patient outcomes require more comprehensive, multipronged interventions in addition to CRM training to have an impact on patient outcomes”.
It’s said that the implementation “of a comprehensive CRM training program in an organization is complicated”. This study was designed with the premise that 3 years post-implementation of the CRM program would be sufficient to pick up on improvements on FTR and mortality; hence, part of the “usual way of doing business”.
They note that while the initial training program was comprehensive, there was no refresher training. Hence, “It is possible that periodic refreshers or booster training for staff is needed to fully sustain, strengthen, and reinforce desired safety behaviors”.
They cite evidence that activities like follow-up debriefings after FTR events to be crucial to effective team comms and maintaining the principles of CRM training in organisations. This CRM intervention didn’t include a standardised post-event debrief as part of its curriculum.
Team size is another potential factor, where “Larger teams have higher levels of collective knowledge, however, smaller teams develop cohesiveness more easily”. They say it’s possible that it was easier for the teams in the non-CRM hospital (control group) to create a cohesive environment due to the smaller facility and fewer team members, thereby enhancing team performance without the CRM intervention.
Overall, they argue that “Maintaining a vibrant culture of safety based on CRM principles in hospitals is challenging, however, participants in CRM training believe that this skillset will improve patient safety”.
While this study didn’t support that contention on FTR and in-hospital mortality, they argue that the “theoretical benefits and the support of some prior studies, the effect of CRM on improving patient care may [still] be positive”.
Authors: Bacon, C. T., McCoy, T. P., & Henshaw, D. S. (2020). Research in Nursing & Health, 43(2), 155-167.
Study link: https://doi.org/10.1002/nur.22007
LinkedIn post: https://www.linkedin.com/pulse/failure-rescue-30-day-in-hospital-mortality-hospitals-ben-hutchinson-rpnyc

One thought on “Failure to rescue and 30-day in-hospital mortality in hospitals with and without crew-resource-management safety training”