I’m currently trying to refresh some of our thinking and approach in prospective learning and investigations; drawing heavily on Leveson’s work (among others).
The attached comes from Leveson’s CAST handbook. Leveson evaluates the Shell Moerdijk Explosion in order to explain her CAST approach (based on STAMP & STPA).
Although all the different hierarchical levels of the Shell and industry systems are evaluated – individuals, teams, plant, operations, management, Shell corporate etc., I found interesting the following focused on operators.
Less interesting are the specific findings in this accident, and more around what questions and threads an investigation should explore.
[Note: I don’t agree with Leveson’s use of “bad decisions” and other judgemental language, but normally she avoids this language]
It’s highlighted that:
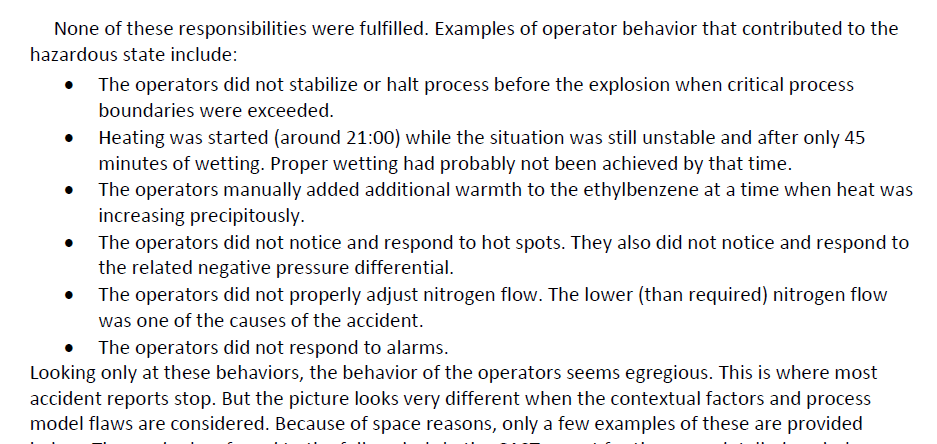
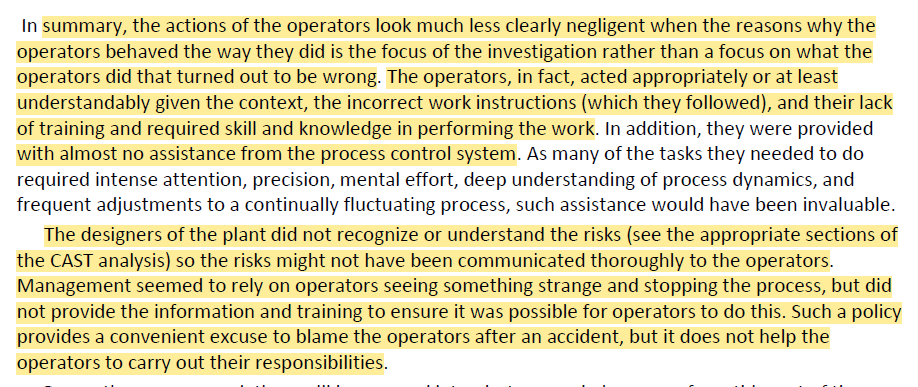
· While investigations are happy to stop at error and human decisions and action with the benefit of hindsight, operators “acted appropriately or at least understandably given the context, the incorrect work instructions (which they followed)” and their mis-calibrated mental models
· Operators weren’t provided with the info they needed, when they needed it to make better informed decisions and the “process control system provided almost no support (feedback)”
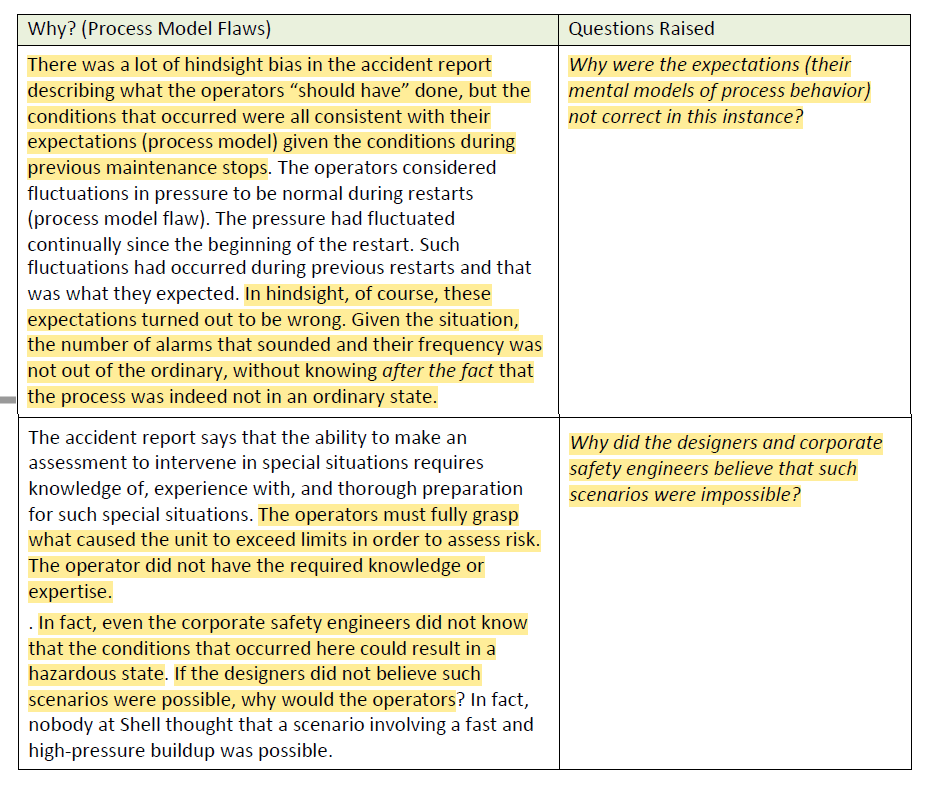
· The tasks also required “intense attention and deep understanding of the process”, prompting questions whether HF analysis done to ensure that operators were capable of manual control, e.g. testing system assumptions
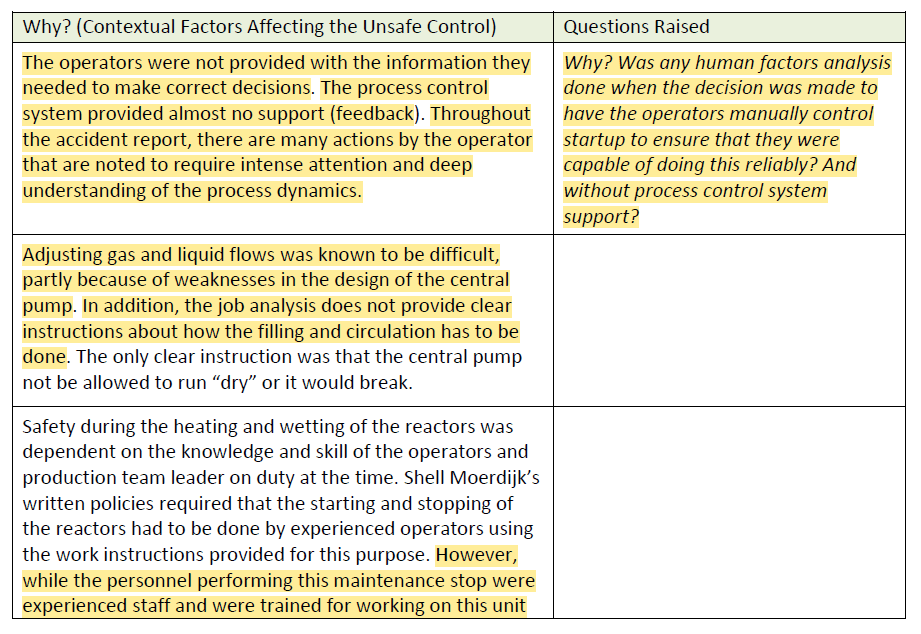
· A design weakness made adjusting gas flows difficult and the job safety analysis “does not provide clear instructions”
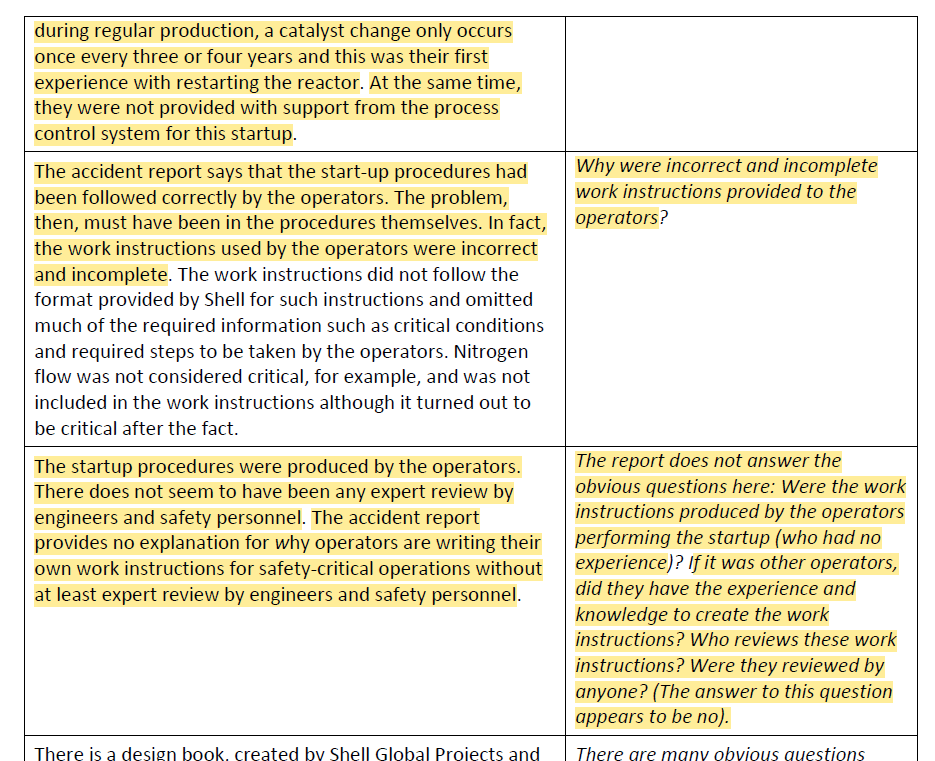
· While staff were experienced for regular production, the catalyst change activity happens only every 3-4 years; affecting expertise, and these operators hadn’t performed a start-up
· “work instructions used by the operators were incorrect and incomplete” and “omitted much of the required information such as critical conditions and required steps to be taken by the operators”
· This prompts questions like how were poor and incomplete procedures provided to operators in the first place?
· The accident report was replete with hindsight bias and counterfactual language, e.g. describing what the operators “should have” done, but providing little context on how those decisions made sense at the time
· E.g., “Why were the expectations (their mental models of process behavior) not correct in this instance?”
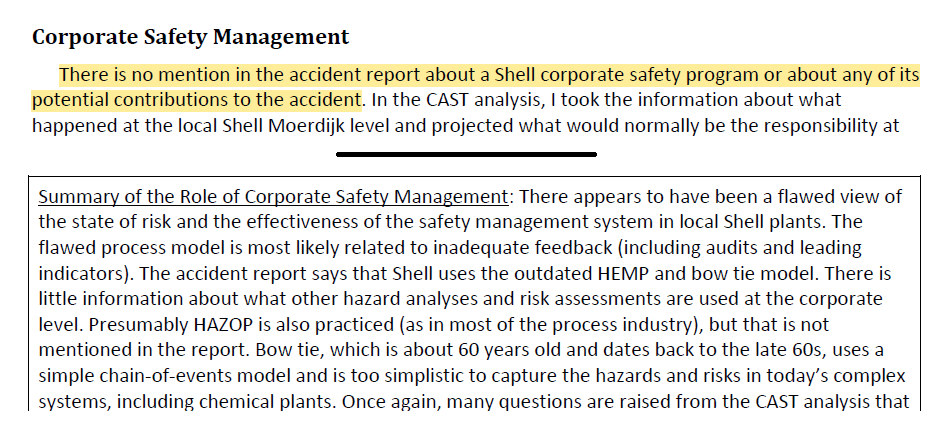
· Issues were also present with design and the corporate safety management system, where “ There appears to have been a flawed view of the state of risk and the effectiveness of the safety management system in local Shell plants”
Ref: CAST HANDBOOK: How to Learn More from Incidents and Accidents Nancy G. Leveson.
Handbook link: http://sunnyday.mit.edu/CAST-Handbook.pdf

2 thoughts on “Better ways to learn from investigations via systems thinking: Leveson and CAST/STAMP/STPA”