What is the role of checklists and time-outs in preventing adverse events? What additional measures are needed to reduce these events?
This brief study, including Sid Dekker and Nancy Leveson, explored these questions in the context of healthcare. I think the general questions and thinking is applicable elsewhere from a systems perspective.
Not a summary – just a few points.
30 adverse events were recorded from a 24-month sample of 380 complex cardiac surgery patients. Nancy Leveson’s CAST technique was used.
They propose that in many ‘conventional’ investigations, mistakes of people are analysed but little other depth is explored; hence, investigations don’t provide the necessary context of local rationality and why people did what they did, and their mental models.
They note that:
· Surgeons’ ‘pick lists’, being their preferred equipment for each surgery, are frequently outdated
· Many physicians are unaware that their preferred equipment are outdated, nor aware of how to change them “suggesting that the surgical leadership team needs to enforce the updating of pick lists”
· Problems were evident with incomplete equipment lists and addressed via investigating the equipment inventory “as opposed to blaming the nurses for not obtaining all of the required equipment”
· There were “important limitations in the use of standard checklists as a stand-alone patient safety measure”
· Major limitations included miscommunication between staff, medication errors, missing instrumentation, missing implants, and improper handling of equipment or instruments
· “Time-outs and checklists can prevent some types of adverse events, but they need to be carefully designed” and “interventions aimed at improving safety controls in the system design are needed to augment the use of checklists”
Some of the arguments in favour of checklists come from their aviation use and supposed influence on low accident rates. However, “the role and impact of checklists on aviation safety have been exaggerated”.
Pilots are said to skip items on checklists, often with the intention of coming back to them; interruptions and distractions influence checklist efficacy; misperception of items; and time constraints.
While checklists do play a role in aviation safety, their role is said to be role in the context of designing fail-safe aircrafts.
Hence, “The success of checklists in aviation depends on the careful analysis and design that go into the entire system design, as well as on human ingenuity in selecting and applying and even modifying standard procedures and checklists”.
Thus, the overuse of checklists “without making system changes is beginning to be recognized in health care too”.
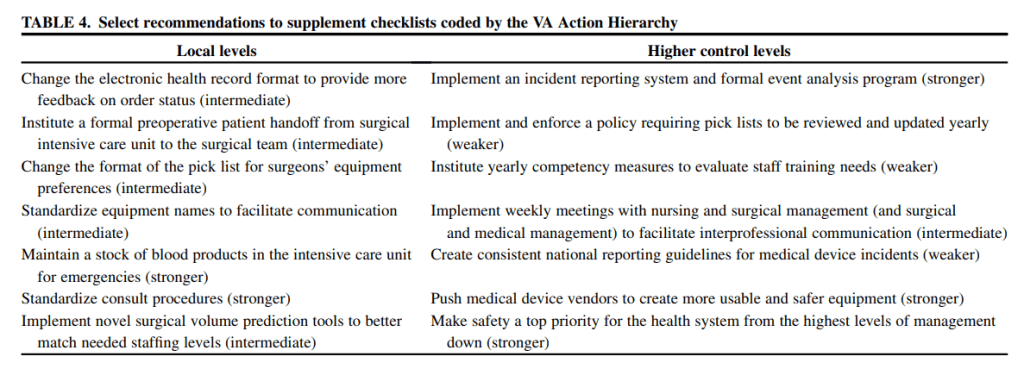
They then provide several improvements based on their CAST analysis, which I’ve skipped.
Study link: https://www.sciencedirect.com/science/article/pii/S0022522316000702
Other checklist studies:
- https://www.linkedin.com/pulse/problem-checklists-ben-hutchinson
- https://www.linkedin.com/pulse/unintended-consequences-checklists-ben-hutchinson
- https://www.linkedin.com/feed/update/urn:li:activity:6930654373064716288?commentUrn=urn%3Ali%3Acomment%3A%28activity%3A6930654373064716288%2C6930654662408761344%29
- https://www.linkedin.com/posts/benhutchinson2_thought-this-attached-guidance-on-developing-activity-7089381291674005504-HejH?utm_source=share&utm_medium=member_desktop
- https://www.linkedin.com/pulse/ritualisation-surgical-safety-checklist-its-from-goals-ben-hutchinson-2buyc

2 thoughts on “When a checklist is not enough: How to improve them andwhat else is needed”