A great read from Jodi Oakman and team exploring who uses ‘how to lift training’ (HTLT) and why.
Importantly “Musculoskeletal disorders (MSDs) have a complex aetiology. How to lift training (HTLT) does not address this complexity, is an ineffective prevention strategy but remains widely utilised”.
1507 survey responses were analysed.
For background:
· In Australia, MSDs account for ~50% of all work-related injuries
· MSDs involve a “complex nature … and substantial evidence underpins the range of psychosocial and physical factors associated with their development”
· MSDs involve biomechanical aspects and psychosocial factors like “decision making latitude and job demands”
· “While variations exist in the effect size of psychosocial hazards on work related MSD risk, the effect size is often comparable to those of biomechanical hazards”
Key findings:
· >70% of participants had used HTLT in an MSD prevention program in the past 2 years
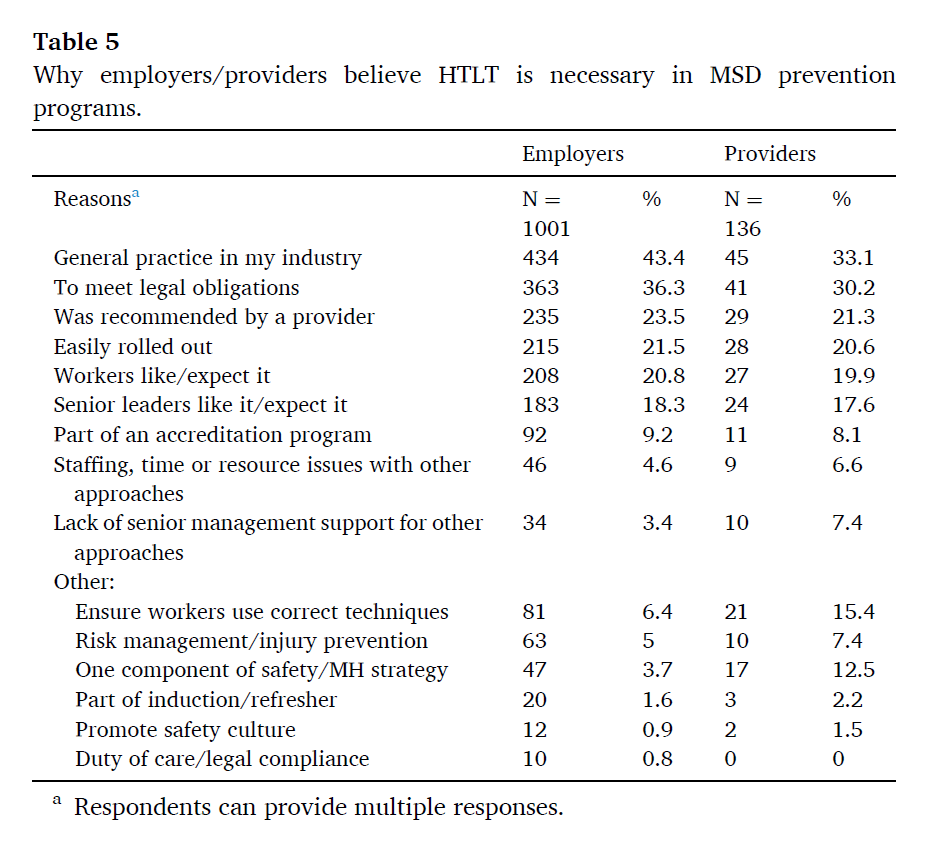
· Employers believed that HTLT is necessary under WHS laws and
providers believed HTLT was a necessary part of MSD prevention
· “The findings from this study suggest several significant evidence to practice gaps in MSD prevention”
· MSDs are said to be “complex disorders caused by exposure to physical and psychosocial workplace hazards”
· Therefore, “Effective prevention of MSDs requires addressing relevant hazards for a particular workplace undertaken within a systems-based management framework which takes into account risk from all hazards together rather than in isolation from each other”
· HTLT “does not meet this requirement, focusing on individual behaviour change through training a worker in how to perform a “safe lifting technique”
· Further, “HTLT while appearing to target the physical aspects of a person’s work does not address most biomechanical risk factors or their source and importantly, does not take into account the broader organisational factors that influence task performance, such as the overall amount of work, or time pressures or autonomy to prioritise tasks”
· The HTLT approach “is focussed on a person’s tasks, rather than their job, and is increasingly being criticised as inadequate for managing the prevention of complex disorders such as MSDs”
· Finally, “A substantial body of strong evidence provides conclusive support that lifting or manual handling techniques training is not an effective means of reducing MSD risk”
Concluding, it’s said that HTLT remains “highly prevalent in MSD prevention despite strong evidence that lifting training is ineffective and does not address WHS legislative requirements”.
Instead, a move towards evidence-based interventions “which take a comprehensive systems-based approach to MSD prevention” is necessary.
Ref: Oakman, J., Lambert, K. A., Rogerson, S., & Bell, A. (2024). International Journal of Industrial Ergonomics, 100, 103542.
Study link: https://doi.org/10.1016/j.ergon.2023.103542
My site with more reviews: https://safety177496371.wordpress.com

One thought on “We know it doesn’t work: Why do we still use how to lift training for the prevention of musculoskeletal disorders?”