Extracts from a paper that studied medication safety in primary care from both a Safety-I and Safety-II lens – using “medication management in the wild” as their data.
· 2 decades after the ‘To Err is Human’ report has “given way to hard bitten realism that there has been little measurable improvement in the overall rates of preventable harm”
· In S-I paradigm, the “dominating approaches pursued in health care have focused on achieving absence of adverse events”, where causation is largely seen as “adverse events in linear, mechanistic manners”
· But these approaches have been criticised for limitations “in recognizing that variations in human performance are needed for success in complex systems”
· S-II “emerged as a paradigm to understand limitations of failure-focused approaches to safety in complex systems”, recognising “that complex systems cannot be decomposed in such a way that safety may be assured by proceduralization of individual components”
· Hence, everyday work in complex systems “must be—variable and flexible to address conditions that are often unexpected and not under the control of frontline workers”
· They observe the “traditional view of quality improvement that almost exclusively measures performance deficiencies, and ignoring the strategies developed by frontline experts” and how this “may have limited added value in primary care medication safety”
· “In complex systems, Safety-I approaches are often not sufficient to reduce harms from ADEs, and one must be mindful that they may impair abilities of clinicians in enacting safety actions … frustrating the agency of frontline workers and increasing risks of burnout”
· And to maximise medication safety “a long list of protocols and rules is not the answer”
· “We are not suggesting that protocols and rules are not necessary, on the contrary they have value if carefully developed and implemented”
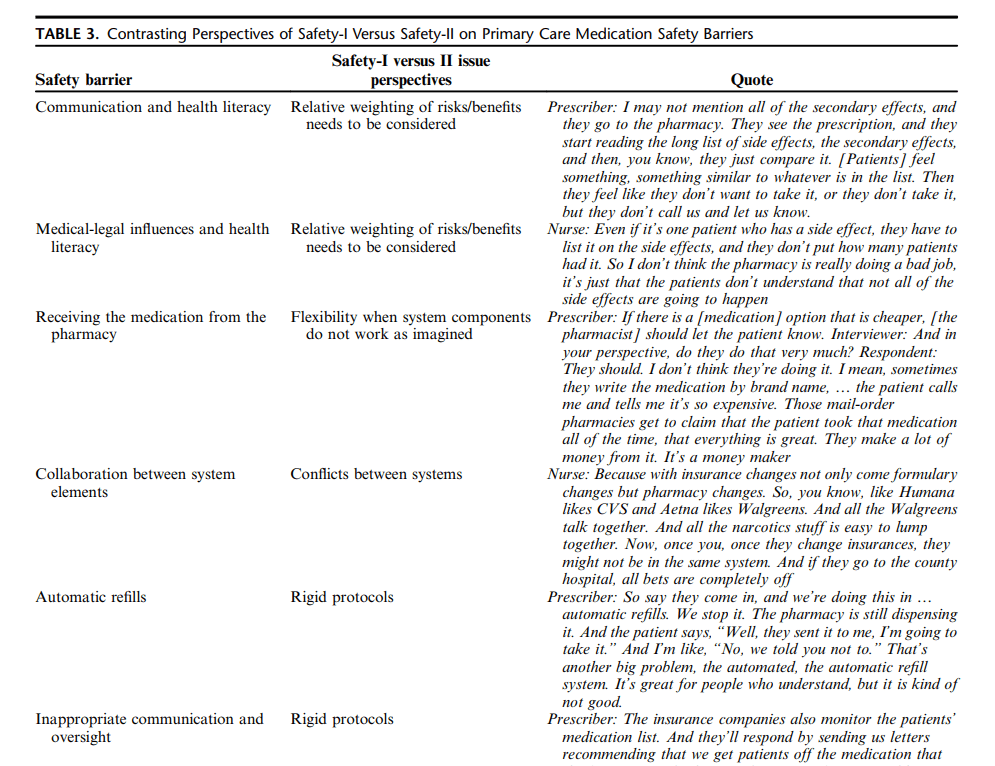
· But, “it should be recognized that there are times when Safety-I and Safety-II principles are in direct conflict”
· If a worker believes that a mandated protocol in their particular circumstance makes no sense, what are they to do? “The Safety-I paradigm means that the worker has no agency, variation in the application of the protocol equals an error, and so the worker should stick to the “best practice,” rather than actually doing the best for a particular patient”
· “The Safety-II paradigm gives the worker agency, who understands the goals of the specific task and the greater organization and is encouraged to create variability to achieve the best outcome”
· “Second, it should be recognized that many procedures or best practices in the Safety-I paradigm are not based on evidence but are driven by the dogma of standardization that can devalue frontline clinicians”
· “The Safety-I paradigm does not recognize that more guidelines may be harmful, or that more standardization may not be desirable. It is the difference between controlling and supporting a complex adaptive sociotechnical system”
· “most primary care-oriented patient safety problems are not amenable to simple solutions and do not match the profound complexity of modern health care settings”
· And “Care is delivered in intricate, fragmented, sometimes chaotic settings, in complex political, sociocultural environments with a virtually infinite range of moving parts and interconnections”
· “These kinds of settings stubbornly resist the introduction of top-down; standardized policy; regulations; or linear-style interventions”
· While “Safety-I assumes that errors can eventually be reduced to an undetectable level”, S-II “assumes that perfect outcomes in a flawless system is an impossible goal”
· “Parts of health care systems are made safer by prioritizing Safety-I principles; others by prioritizing Safety-II principles. The best system strikes a balance between the two”
Ref: Young, R. A., Xiao, Y., Fulda, K. G., White, A., & Gurses, A. P. (2025). Journal of Patient Safety, 21 (7Supp), S81-S88.

Study link: https://doi.org/10.1097/PTS.0000000000001400
Safe As LinkedIn group: https://www.linkedin.com/groups/14717868/
