This study explored safety practices perceived as low value in healthcare.
Data came from 1041 participants across Australia & the UK.
They argue that this is an important area to unpack given the prevalence of safety clutter, and research highlight the extent of “ineffective practices and systemic waste in healthcare services, with evidence that up to 30% of healthcare provision is unnecessary”.
PS. Check out my YouTube channel. Link in comments
Results
They identified several themes of low value practices.
1. Blanket policies
Blanket policies are procedures applied across patient groups and not adapted to suit individual patient needs.
While blanket policies are implemented to counter preventable adverse events (e.g. thromboembolism), some participants “perceived mandatory completion of such checks on patients at very low risk to be a waste of time”.
An example being a blanket policy to undertake falls assessments, which have little perceived value for patients with obviously very low-risk of falls.
Some blanket policies may waste staff time and also lead to harm when carried out on particular patients who are unlikely to benefit.
Others considered a task to be unnecessary because it didn’t have a visible effect on patient safety, but still had to be done due to policy, for instance “Doing tasks because the standards say so, rather than it’s of benefit to care”.
2. Covering Ourselves
Some admin tasks were said to be a waste of time because they took staff time away from providing direct care, instead to “produce evidence of completed safety-related tasks (e.g., safety checklists)”.
While many participants recognised what the intention of the admin process was, e.g. reducing the risk of adverse events, “they also conveyed beliefs that the volume of administrative tasks meant that this strategy had become counterproductive, potentially detracting from rather than enhancing patient safety”.
An example was filling in multiple forms to indicate that care was done. In these cases, “forms become more important than doing the care”.
Others perceived these activities to be more about reducing legal risk in the event of a serious incident, rather than on increasing patient safety. One participant observed that ““Obsessive admin[istration] doesn’t change patient care but does cover our backs—at the cost of time”.
3. Not My Job
Another theme related to staff performing tasks outside the scope of practice, which takes time away from their core caring responsibilities.
Some reported that some of these tasks should be allocated to other staff with more appropriate skill sets, to ensure that more specialised healthcare professionals have adequate time on tasks that require their expertise. An example was controlled drugs checks – which was suggested could be performed entirely by pharmacists.
4. Approaches to Implementation of Safety Practices
Some practices depending on their implementation can detract from patient safety. For instance a particular policy carried out according to guidelines may enhance safety, but if that policy is implemented without appropriate guidance or support, then may lead to more harm than good.
5. Lack of Impact
This theme relates to how some practices “be a waste of time if they do not lead to discernible action or change”. E.g. “…writing these (local operating procedures)…makes no difference … it’s just another thing to read”.
Activities that staff have to perform without clear benefits affects motivation. Another example is completing an audit without implementing a plan for positive change.
Some activities, including audits and inspections, can tell “ staff that we are doing poorly at things and rarely has positive benefits or enforcement of better behaviors”. Hence, some activities are perceived as low value because they “induce negative feelings among staff that are not conducive to facilitating improvements in care”.
Conclusion
Summing up what they found:
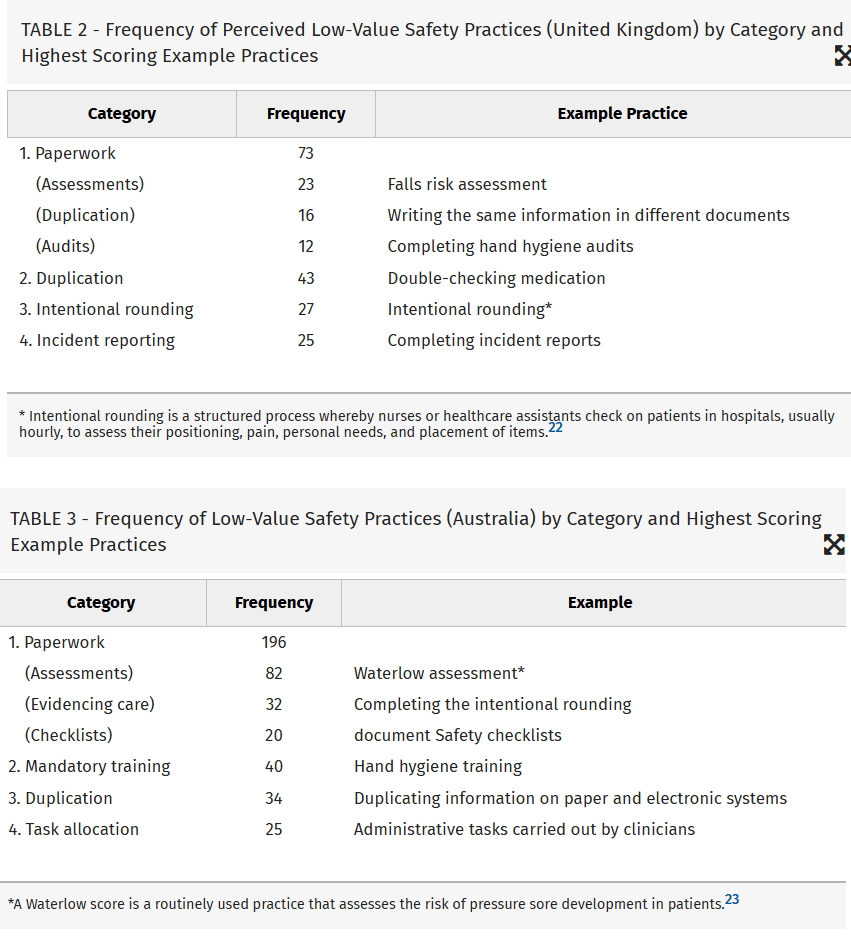
· Paperwork was perceived by staff as the greatest “waste of time”
· Duplication was also perceived by staff as low value, with double checking medication being the most commonly identified item
· Incident reporting was also frequently mentioned as a low value activity
· They note that the value of incident reporting “has been questioned repeatedly … [and] although well intended, and central to many efforts to improve healthcare safety, suffers from a variety of limitations, including physician underreporting and, when incidents are reported, visible action in response to these is rare”
· They discuss double checking of medicines, noting that some research has found that double checking makes healthcare professionals feel safer when administering these meds in high-risk situations, but also requires additional resourcing and causes workflow interruptions which may introduce other risks
· Mandatory training was also seen as a low value activity, for instance hand washing
Interestingly, they argue that “Rather than investigating whether this practice is appropriate for deimplementation [i.e. removal], it would be more useful to explore why healthcare staff perceived hand hygiene training to be low value and how it can be modified to become less onerous” (emphasis added).
Ref: Halligan, D., Janes, G., Conner, M., Albutt, A., Debono, D., Carland, J., … & Lawton, R. (2023). Identifying safety practices perceived as low value: An exploratory survey of healthcare staff in the United Kingdom and Australia. Journal of Patient Safety, 19(2), 143-150.
LinkedIn post: https://www.linkedin.com/pulse/identifying-safety-practices-perceived-low-value-ben-hutchinson-phd–4lnce
