
This study redesigned the hierarchy of controls (HoC) to target workplace psychosocial hazards, specifically, adapting the NIOSH Total Worker Health HoC.
These called this the Psychosocial Hierarchy of Control (P-HoC). Won’t be anything earth shattering for most, but nice to see it properly articulated.
For background:
· “There is consistent evidence that psychosocial hazards at work are contributing to various health problems such as mental disorders, cardiovascular diseases, and musculoskeletal health”
· “the WHO estimates that 15% of working‐age adults have a mental disorder at any point in time and that this costs the global economy US$ 1 trillion each year due to lost productivity”
· “There is evidence that work can cause or exacerbate mental health conditions [1, 2]. Similarly, it is well established that psychosocial hazards at work have a substantial effect on musculoskeletal health; the main contributor to disability worldwide”
· “Psychosocial aspects of work include, among other factors, job content, workload and work pace, work schedule, and organizational culture, which all have associated psychosocial hazards”
Results
Below is their P-HoC:
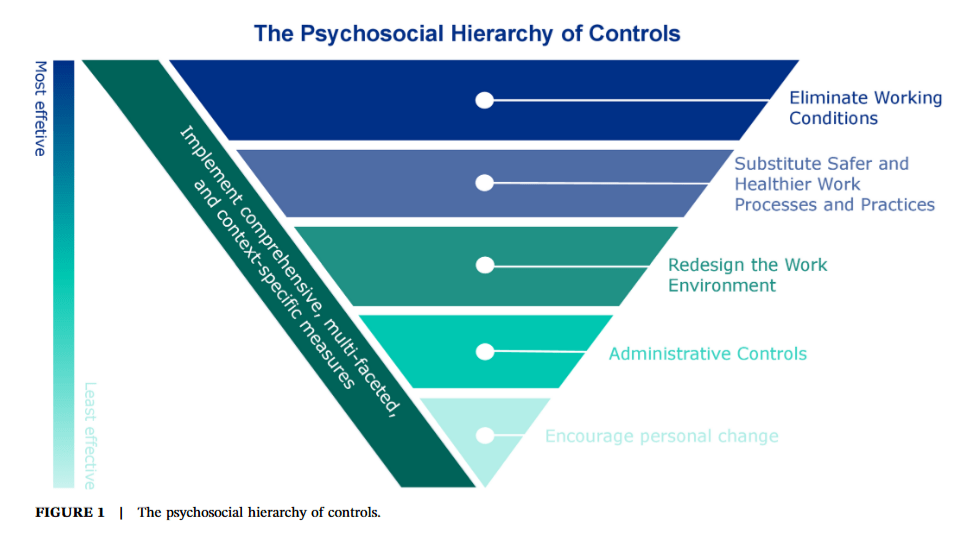
And it contains the following justifications:

They discuss the degree of evidence between organisational vs individual-level psychosocial interventions. First, while organisational-level interventions are recommended for the prevention of stress and some other psychosocial factors, “systematic reviews show that these interventions do not always have the intended outcomes”.
Why organisation-level interventions may not always be effective may be explained by “the fact that organizations are complex systems and the success of the interventions is influenced by the internal and external organizational context, the intervention and its implementation, and the participants’ perception of the intervention”.
Some interventions have been found to be effective though: interventions to reduce workload or increasing their time or resources. Changing their working time arrangements, including more control over their shift scheduling, also have positive effects on work outcomes.
In contrast, more consistent evidence exists for the effectiveness of individual-level interventions, and this likely because “studying the effects of individual interventions is more accessible; companies are generally more reluctant to implement organizational interventions which may be more costly, time‐consuming, or change‐oriented”. Hence, individual-level interventions are easier and more plentiful to study.
So while there is stronger evidence for individual focus, “this does not necessarily represent the primary drivers of a healthy psychosocial working environment”. The authors argue that organisational-level interventions should be the core focus, in alignment with the existing HoC.
Higher-level interventions and preventative measures “create systemic changes that benefit all workers”.
Admin measures should likewise be placed at the lower end of the hierarchy; although they can and are still useful, like for communicating and raising awareness.
At the highest-level, interventions focus on directly reducing employee workload, increasing their time or resources, and therefore “reduce the quantitative demands of work”, in alignment with the elimination principle.
They note that as with the existing HoC, not all hazards can be eliminated.
Level 4 focuses on changing working time arrangements, preferably by giving employees more control on scheduling their work time.
Level 3 is aligned with NIOSH’s Total Worker Health HoC about “redesign the work environment for safety, health, and well‐being’”. This emphases organisational measures like management support, and redesigning the physical or organisational environment.
At level 1, individual measures like mindfulness, information, psyche therapies and more are placed. While these can be effective at stress reduction, they “should be viewed as supplementary to comprehensive organizational strategies”.
Like the HoC, the P-HoC places “personal change … on the lowest level of the hierarchy”.
Discussion
Discussing the logics, they say that organisations often focus on admin and individual level interventions since they’re easier to implement. Org level interventions are of course more difficult or complicated (perhaps complex), and “more likely to encounter contextual and procedural factors that hinder their success”.
They also argue that, perhaps, another motivation for individual-level and admin interventions “as proposed by Rae and Provan (2019), [is] that the measures can serve the purpose of ‘demonstrated safety’”.
Ref: Kjærgaard, A., Rudolf, E. M., Palmqvist, J., Jakobsen, M. E., & Ajslev, J. Z. N. (2025). The psychosocial hierarchy of controls: effectively reducing psychosocial hazards at work. American Journal of Industrial Medicine, 68(3), 250-263.

Study link: https://doi.org/10.1002/ajim.23694
LinkedIn post: https://www.linkedin.com/pulse/psychosocial-hierarchy-controls-effectively-reducing-work-hutchinson-w4ddc
